| S1: |
For more informed treatment decisions in mNSCLC, wait for all biomarker test results |
| S2: |
Are you leveraging biomarker test results in mNSCLC? |
| S3: |
Why it is important to wait for all biomarker test results in mNSCLC |
| S4: |
Is targeted therapy an option for your mNSCLC patients? |
| S5: |
Following up on our conversation about biomarker testing in mNSCLC |
| S6: |
Are you available to talk about the importance of biomarker testing in mNSCLC? |
|
| Preheader: |
Biomarker test results may help optimize treatment plans in mNSCLC |
|
[From: <Rep Name> (REPNAME@blueprintmedicines.com)]
[Sent: <MM/DD/YYYY HH:MM AM/PM>]
[To: <Last Name, First Name>]
|

|
|
[pick list]
[Dear]
[Hello]
[pick list]
[Dr. Last Name],
[First Name],
[First Name Last Name],
|
|
[Customize the text here with your own message to the healthcare provider in alignment with FDM. You may only send a 200-character message in alignment with FDM.]
|
|
The importance of obtaining complete biomarker test
results prior to initiating first-line therapy in mNSCLC
|
|
Insufficient tissue (or QNS) is not a conclusive result. Consider retesting to determine if a biomarker is present.1
|
|
|
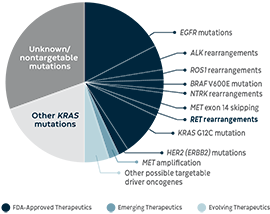
About 1 in 2 patients with mNSCLC have biomarkers with approved, emerging, or evolving therapeutics1,2
|
|
|
|
RET fusions are 1 of 9 driver alterations with FDA-approved therapies1,2
|
|
In pivotal studies, patients with RET+ mNSCLC have been shown to respond to RET inhibitors across all lines of therapy, including first line.3
|
|
Ensure you review all biomarker test results before making therapeutic decisions2,3
|
|
Emerging Therapeutics=currently being studied in clinical trials; Evolving Therapeutics=either proof-of-concept studies or in a very early clinical stage.
|
|
|

|
|
Although many mNSCLC patients have derived benefit from immunotherapy (IO), some biomarker-driven cancers may respond poorly to IO treatment4-7
|
| • |
mNSCLC patients with biomarkers are often excluded from IO clinical trials5,8 |
| • |
In a retrospective study of 551 advanced NSCLC patients, IO response rates in select biomarker-driven NSCLC were4*:
|
– ALK (n=23): 0%
|
|
– BRAF (n=43): 24%
|
|
– EGFR (n=125): 12%
|
|
– HER2 (ERBB2) (n=29): 7%
|
|
– KRAS (n=271): 26%
|
|
– MET (n=36): 16%
|
|
– RET (n=16): 6%
|
|
– ROS1 (n=7): 17%
|
|
|
|
|
| * |
IO response rates reflect best overall response (defined as a complete or partial response occurring at least once during treatment, according to RECIST v1.1 criteria). |
|
|

|
|
Before administering first-line immunotherapy, consider these recommendations from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Non-Small Cell Lung Cancer1:
|
| • |
Across all PD-L1 expression levels, the NCCN Guidelines® recommend that patients are negative for actionable molecular markers before utilizing immunotherapy as a first-line treatment option for mNSCLC† |
| • |
Contraindications for treatment with PD-1/PD-L1 inhibitors in patients with advanced or metastatic NSCLC may include the presence of oncogenes (such as EGFR, ALK, and RET), which would predict a lack of benefit
|
|
|
|
| † |
The NCCN Guidelines for NSCLC provide recommendations for certain individual biomarkers that should be tested and recommend testing techniques, but do not endorse any specific commercially available biomarker assays or commercial laboratories. |
|
See the NCCN Guidelines for NSCLC for detailed recommendations, including preferred treatment options. NCCN makes no warranties of any kind whatsoever regarding their content, use, or application, and disclaims any responsibility for their application or use in any way. |
|
ALK=anaplastic lymphoma kinase; BRAF=B-Raf proto-oncogene; EGFR=epidermal growth factor receptor; ERBB2=erb-b2 receptor tyrosine kinase 2; HER2=human epidermal growth factor receptor 2; KRAS=Kirsten rat sarcoma; MET=MET proto-oncogene; mNSCLC=metastatic non–small cell lung cancer; NCCN=National Comprehensive Cancer Network®; NTRK=neurotrophic tyrosine receptor kinase; PD-1=programmed cell-death protein 1; PD-L1=programmed death-ligand 1; QNS=quantity not sufficient; RECIST=Response Evaluation Criteria in Solid Tumors; RET=rearranged during transfection; ROS1=ROS proto-oncogene 1. |
|
|
|
|
| I’ve included some information I hope you’ll find useful. |
[Fragment/attachment pick list]
|
[Biomarker Testing and Treatment Initiation Flashcard]
|
|
|
|
|
|
| I’m available in person or virtually to answer any questions you may have. |
[pick list]
[Sincerely],
[Best],
|
|
[Rep photo]
|
[pick list]
[Rep name]
[Rep title]
Blueprint Medicines
[Rep phone number]
[Rep email address]
|
|
|
|
|
References:
1. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Non-Small Cell Lung Cancer V.5.2022. © National Comprehensive Cancer Network, Inc. 2022. All rights reserved. Accessed October 5, 2022. To view the most recent and complete version of the guideline, go online to NCCN.org.
2. VanderLaan PA, Rangachari D, Costa DB. The rapidly evolving landscape of biomarker testing in non–small cell lung cancer. Cancer Cytopathol. 2021;129(3):179-181.
3. Drusbosky LM, Rodriguez E, Dawar R, Ikpeazu CV. Therapeutic strategies in RET gene rearranged non-small cell lung cancer. J Hematol Oncol. 2021;14(50):1-8.
4. Mazières J, Drilon A, Lusque A, et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: results from the IMMUNOTARGET registry. Ann Oncol. 2019;30(8):1321-1328.
5. Addeo A, Passaro A, Malapelle U, Banna GL, Subbiah V, Friedlaender A. Immunotherapy in non-small cell lung cancer harbouring driver mutations. Cancer Treat Rev. 2021;96:102179. doi:10.1016/j.ctrv.2021.102179.
6. Chen R, Tao Y, Xu X, et al. Discov Med. 2018;26(143):155-166.
7. Lisberg A, Cummings A, Goldman JW, et al. J Thorac Oncol. 2018;13(8):1138-1145.
8. Offin M, Guo R, Wu SL, et al. Immunophenotype and response to immunotherapy of RET-rearranged lung cancers. JCO Precis Oncol. 2019;3:PO.18.00386. doi:10.1200/PO.18.00386.
|
|
|
|
|
