|
|
| P1: |
Review the updated efficacy and safety data |
|
[From: <Rep Name> (REPNAME@blueprintmedicines.com)]
[Sent: <MM/DD/YYYY HH:MM AM/PM>]
[To: <Last Name, First Name>]
|
|
|

|
|
[pick list]
[Dear]
[Hello]
[pick list]
[Dr. Last Name],
[First Name],
[First Name Last Name],
|
|
[Customize the text here with your own message to the healthcare provider in alignment with the Field Direction Memo (FDM). You may only send a 200-character message in alignment with the FDM. The message must be limited to a greeting and may not contain any implied/expressed product claims.]
|
|
I’m excited to share that updated pivotal data for GAVRETO® (pralsetinib), which is based on a larger patient population, continues to demonstrate a
robust and durable response in RET+ mNSCLC. GAVRETO is the only once-daily targeted RET therapy indicated for adult patients with RET
fusion+ mNSCLC as detected by an FDA-approved test.1
|
|
Please review the updated pivotal data, including ORR, DoR, CNS activity, safety, and more, provided below. If you’d like to set up a
[pick list]
[falsecalltruevideo chattruemeeting]
to go over the data, or if you have any questions about GAVRETO, please let me know.
|
|
CNS=central nervous system; DoR=duration of response; mNSCLC=metastatic non–small cell lung
cancer; ORR=overall response rate; RET+=rearranged during transfection positive.
|
|
SELECT SAFETY INFORMATION
|
|
Serious and sometimes fatal adverse reactions occurred with GAVRETO. Warnings and precautions include interstitial lung disease/pneumonitis,
hypertension, hepatotoxicity, hemorrhagic events, tumor lysis syndrome, risk of impaired wound healing, and embryo-fetal toxicity.
|
|
Please see additional Important Safety Information below and full Prescribing Information.
|
|
GAVRETO continues to demonstrate a robust and durable response in RET+ mNSCLC1
|
|
Efficacy and safety with GAVRETO (400 mg orally once daily) were evaluated in patients with RET fusion+ mNSCLC in the ARROW study, a
phase 1/2, nonrandomized, open-label, single-arm, multicohort, multicenter clinical trial.1,2 Patients with asymptomatic CNS metastases, including
patients with stable or decreasing steroid use within 2 weeks prior to study entry, were enrolled.1
|
|
The major efficacy outcome measures were ORR and DoR, as assessed by a BICR according to RECIST v1.1.1
|
|
BICR=blinded independent central review; RECIST=Response Evaluation Criteria in Solid Tumors.
|
|
Efficacy results in treatment-naïve patients1
|
|
Overall Response Rate (n=107)
|

|
|
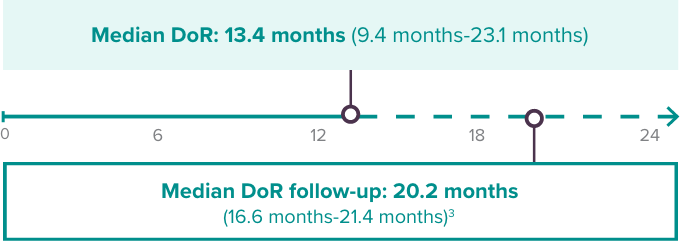
Duration of and Time to Response (n=83)
|
|
 |
45% of patients continued to respond to treatment at ≥12 months* |
|
Median time to first response was 1.8 months (range: 0.9 months-6.1 months)3 |
|
|
Efficacy results in previously platinum-treated patients1
|
|
Overall Response Rate (n=130)
|

|
|
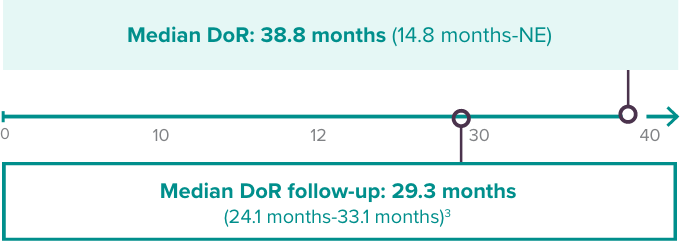
Duration of and Time to Response (n=82)
|
|
|
66% of patients continued to respond to treatment at ≥12 months* |
|
Median time to first response was 1.8 months (range: 1.3 months-11.4 months)3 |
|
|
Patients enrolled by July 11, 2019. Data cutoff: March 4, 2022.
|
|
*Based on observed DoR.
|
|
CI=confidence interval; CR=complete response; NE=not estimable; PR=partial response.
|
|
SELECT SAFETY INFORMATION
|
|
Interstitial Lung Disease (ILD)/Pneumonitis: Severe, life-threatening, and fatal ILD/pneumonitis can occur in patients treated with GAVRETO.
Pneumonitis occurred in 12% of patients who received GAVRETO, including 3.3% with Grade 3-4, and 0.2% with fatal reactions. Monitor for
pulmonary symptoms indicative of ILD/pneumonitis. Withhold GAVRETO and promptly investigate for ILD in any patient who presents with acute or
worsening of respiratory symptoms (e.g., dyspnea, cough, and fever). Withhold, reduce dose or permanently discontinue GAVRETO based on
severity of confirmed ILD.
|
|
Please see additional Important Safety Information below and full Prescribing Information.
|
 |
GAVRETO demonstrated CNS activity in previously treated patients with measurable brain metastases1
|
|
|
Brain metastases at baseline (n=10)†:
|

|
|
†No patients received radiation therapy (RT) to the brain within 2 months prior to study entry.
|
|
Adverse reactions in RET+ mNSCLC (n=281)1
|
|
Serious adverse reactions occurred in 65% of patients who received GAVRETO. The most frequent serious adverse reactions (in ≥2% of
patients) were pneumonia, anemia, pneumonitis, pyrexia, sepsis, urinary tract infection, coronavirus infection, pleural effusion, dyspnea,
musculoskeletal pain, pulmonary embolism, and seizure. Fatal adverse reactions occurred in 7% of patients; fatal adverse reactions that occurred in
>1 patient included pneumonia (n=8), sepsis (n=3), and COVID (n=3).
|
|
Adverse reactions (≥15%) were constipation (45%), edema‡ (44%), musculoskeletal pain‡ (44%), fatigue‡ (42%), hypertension‡ (38%),
cough‡ (36%), diarrhea (30%), pyrexia (29%), pneumonia‡ (24%), dyspnea (21%), increased blood creatine phosphokinase (19%), nausea
(19%), decreased appetite (18%), dry mouth (17%), rash‡ (17%), taste disorder‡ (17%), urinary tract infection (16%), and headache‡ (15%).
|
|
‡For grouped terms, please refer to the U.S. Prescribing Information (USPI).
|
|
I’ve included some additional resources you may find useful:
|
|
|
[Fragment/attachment pick list]
|
|
[pick list]
[Sincerely],
[Best],
|
|
|
|
|
Hypertension: Occurred in 35% of patients, including Grade 3 hypertension in 18% of patients. Overall, 8% had their dose interrupted and 4.8% had their
dose reduced for hypertension. Treatment-emergent hypertension was most commonly managed with anti-hypertension medications. Do not initiate GAVRETO in patients with uncontrolled hypertension. Optimize blood
pressure prior to initiating GAVRETO. Monitor blood pressure after 1 week, at least monthly thereafter and as clinically indicated. Initiate or adjust anti-hypertensive
therapy as appropriate. Withhold, reduce dose, or permanently discontinue GAVRETO based on the severity.
|
|
Hepatotoxicity: Serious hepatic adverse reactions occurred in 1.5% of patients treated with GAVRETO. Increased aspartate aminotransferase (AST)
occurred in 49% of patients, including Grade 3 or 4 in 7% and increased alanine aminotransferase (ALT) occurred in 37% of patients, including Grade 3 or 4 in 4.8%. The median time to first onset for increased AST was 15 days
(range: 5 days to 2.5 years) and increased ALT was 24 days (range: 7 days to 3.7 years). Monitor AST and ALT prior to initiating GAVRETO, every 2 weeks during the first 3 months, then monthly thereafter and as clinically indicated.
Withhold, reduce dose or permanently discontinue GAVRETO based on severity.
|
|
Hemorrhagic Events: Serious, including fatal, hemorrhagic events can occur with GAVRETO. Grade ≥3 events occurred in 4.1% of patients treated with
GAVRETO including one patient with a fatal hemorrhagic event. Permanently discontinue GAVRETO in patients with severe or life-threatening hemorrhage.
|
|
Tumor Lysis Syndrome (TLS): Cases of TLS have been reported in patients
with medullary thyroid carcinoma receiving GAVRETO. Patients may be at risk of TLS if they have rapidly growing tumors, a high tumor
burden, renal dysfunction, or dehydration. Closely monitor patients at risk, consider appropriate prophylaxis including hydration, and treat as clinically indicated.
|
|
Risk of Impaired Wound Healing: Impaired wound healing can occur in patients who receive drugs that inhibit the vascular endothelial growth factor
(VEGF) signaling pathway. Therefore, GAVRETO has the potential to adversely affect wound healing. Withhold GAVRETO for at least 5 days prior to elective surgery. Do not administer for at least
2 weeks following major surgery and until adequate wound healing. The safety of resumption of GAVRETO after resolution of wound healing complications has not been established.
|
|
Embryo-Fetal Toxicity: Based on findings from animal studies and its mechanism of action, GAVRETO can cause fetal harm when administered to a
pregnant woman. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective non-hormonal contraception during treatment with GAVRETO and for 2 weeks after the last
dose. Advise males with female partners of reproductive potential to use effective contraception during treatment with GAVRETO and for 1 week after the last dose.
|
|
Common adverse reactions (≥25%) were musculoskeletal pain, constipation, hypertension, diarrhea, fatigue, edema, pyrexia, and cough.
Common Grade 3/4 laboratory abnormalities (≥2%) were decreased lymphocytes, decreased neutrophils, decreased hemoglobin, decreased phosphate, decreased leukocytes, decreased sodium, increased aspartate
aminotransferase (AST), increased alanine aminotransferase (ALT), decreased calcium (corrected), decreased platelets, increased alkaline phosphatase, increased potassium, decreased potassium, and increased bilirubin.
|
|
Avoid coadministration of GAVRETO with strong or moderate CYP3A inhibitors, P-gp inhibitors, or combined P-gp and strong or moderate
CYP3A inhibitors. If coadministration cannot be avoided, reduce the GAVRETO dose. Avoid coadministration of GAVRETO with strong or
moderate CYP3A inducers. If coadministration cannot be avoided, increase the GAVRETO dose.
|
|
Lactation: Advise women not to breastfeed during treatment with GAVRETO and for 1 week after the last dose.
|
|
Pediatric Use: Monitor open growth plates in adolescent patients. Consider interrupting or discontinuing GAVRETO if abnormalities occur.
|
|
You may report side effects to the FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. You may also report side effects to Genentech at 1-888-835-2555.
|
|
Please click here to see the full Prescribing Information and Patient Information for GAVRETO.
|
|
GAVRETO is indicated for the treatment of adult patients with metastatic rearranged during transfection (RET) fusion-positive non-small cell lung cancer (NSCLC) as detected by an FDA-approved test.
|
|
References: 1. GAVRETO Prescribing Information. Genentech, Inc. August 2023.
2. Phase 1/2 study of the highly-selective RET inhibitor, pralsetinib (BLU-667), in patients with thyroid cancer, non-small
cell lung cancer, and other advanced solid tumors (ARROW). ClinicalTrials.gov identifier:
NCT03037385. https://clinicaltrials.gov/ct2/show/NCT03037385. Accessed September 5, 2023.
3. Data on file. Blueprint Medicines Corporation. Cambridge, MA; 2022.
|
|
|
|
|
|