[Subject Line Options - choose one]
| OPTION 1: |
Let’s talk 1:1 about a treatment for Fabry disease |
| OPTION 2: |
A treatment option for your Fabry patients |
| OPTION 3: |
Have you heard about this treatment for Fabry disease? |
| OPTION 4: |
Exciting news for your patients with Fabry disease |
[Preheader - only one can be used, not selectable]
| Preheader: |
Key info about an ERT for Fabry |
| From: |
[{{userName}} <{{RepEmailAddress}}>] |
| Reply To: |
[{{userName}} <{{RepEmailAddress}}>] |
| Sent: |
[<MM/DD/YYYY HH:MM AM/PM>] |
| To: |
[Last Name, First Name <email address>] |
|
If your email program has trouble
displaying this email, view it as a web page.
|
|
Full Prescribing Information
|

|

|
Picture what long-lasting treatment can do1,2*
For your ERT-experienced and
treatment-naïve patients:
The PEGylated ERT for Fabry1,2 
|
|

|

|
{{customText [falseHitrueHellotrueDeartrueGreetingstrueGood morningtrueGood afternoontrueGood evening]}}
{{customText [false##accTitle## ##accFname## ##accLname##true##accTitle## ##accLname##true##accFname##]}},
{{customText
[falseI want to thank you for our discussion about Elfabrio.trueI want to thank you for our meeting about Elfabrio.trueI want to thank you for requesting more info on Elfabrio.trueI’m sorry we weren’t able to connect about Elfabrio.trueI wanted to share this information about Elfabrio with you.]}}
|
The efficacy and safety of Elfabrio were validated by a robust, broad-ranging clinical trial program in Fabry disease, including adult male and female switch and treatment-naïve patients with classic or nonclassic Fabry.1,3-6 I’d like to share more information with you about the clinical profile and the important features of Elfabrio.
| * |
Elfabrio has an initial half-life of 78.9 ± 10.3 hours. Clinical studies have not established that pharmacological characteristics, including half-life, result in superior efficacy or safety based on clinically relevant endpoints.1 |
| ERT, enzyme replacement therapy; PEG, polyethylene glycol. |
|
FRAGMENT [Why Elfabrio?]
|
Reasons why Elfabrio may be right for your patients:

|
|
|
See the clinical trial results
|
| † |
Clinical studies have not established that pharmacological characteristics, including half-life, result in superior efficacy or safety based on clinically relevant endpoints. |
| ‡ |
The effect of IgG ADAs on the effectiveness of Elfabrio has not been fully characterized. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. |
| ADAs, anti-drug antibodies; eGFR, estimated glomerular filtration rate; IgG, immunoglobulin G. |
|
|
FRAGMENT [Head-To-Head Study]
|
Studied head-to-head vs agalsidase beta1,3
The efficacy and safety of Elfabrio, 1 mg/kg every 2 weeks, vs agalsidase beta were studied in BALANCE, a head-to-head, randomized, double-blind, 2-year, active-controlled study.1,3
| • |
Prior agalsidase beta: >1 year, average of 5.7 years
|
| • |
Primary study: 24 months (n=78, ITT=77, PP=72)
|
| • |
Open-label extension: Up to 60 months
|
Primary endpoint1,3
| • |
Annualized rate of change in eGFR (eGFR slope) assessed over 2 years
|
Safety endpoints3
| • |
Treatment-emergent adverse events, infusion-related reactions, anti-drug antibodies
|
BALANCE (Trial 2 in the Elfabrio Prescribing Information) provided confirmatory evidence in the FDA’s approval of Elfabrio. The data discussed are not intended to establish noninferiority or superiority to any other marketed drug product on the basis of safety or efficacy.5†
| † |
|
| eGFR, estimated glomerular filtration rate; FDA, Food and Drug Administration; ITT, intention to treat; PP, per protocol. |
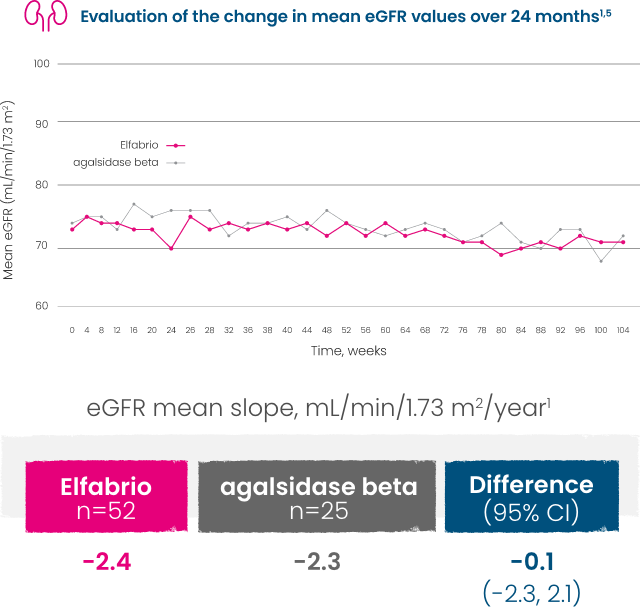
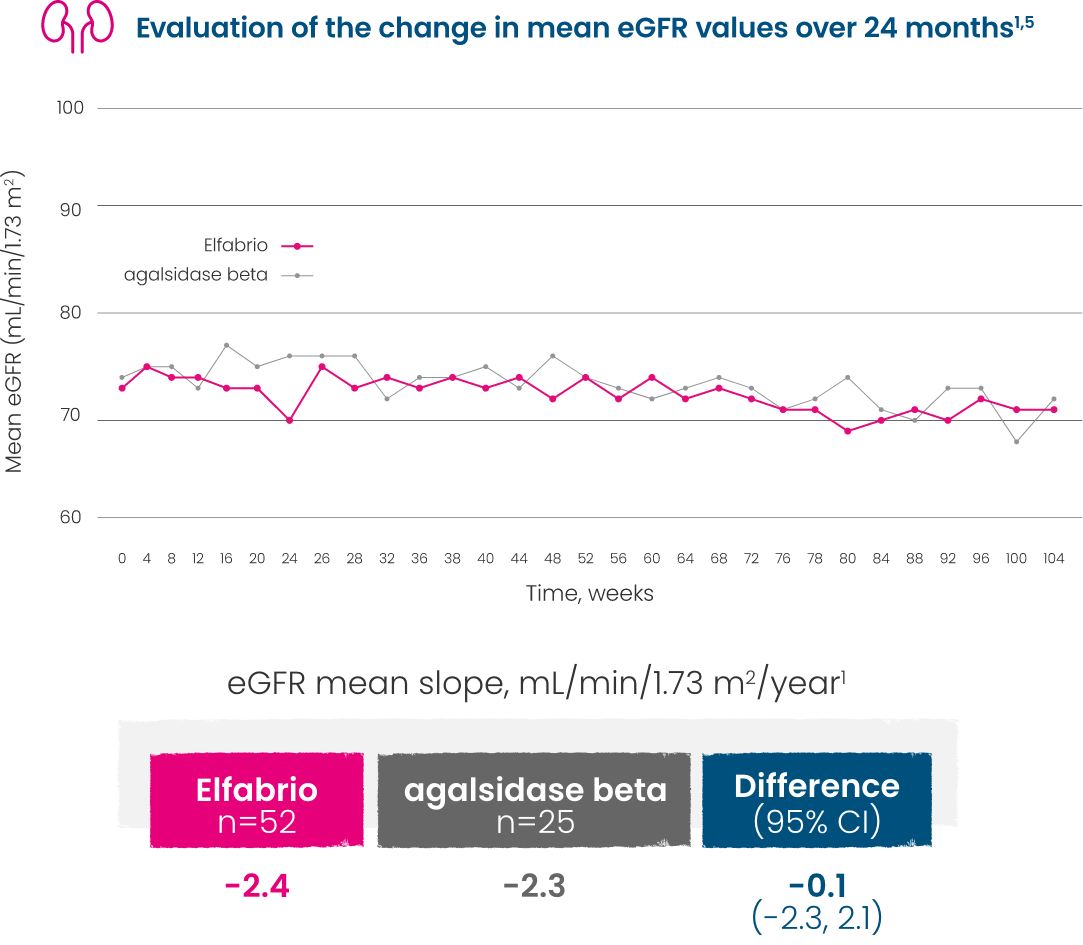
Comparable effect on eGFR vs agalsidase beta over 2 years1,5
The comparable effect on eGFR aligns with the FDA’s determination that the slopes in each arm were comparable based on a series of supportive statistical analyses.
The FDA has indicated that the magnitude of drug effect of agalsidase beta in a study population similar to that of BALANCE (Trial 2 in the Elfabrio Prescribing Information) cannot be sufficiently quantified and as such, a noninferiority margin cannot be determined for BALANCE.
CI, confidence interval.
|
FRAGMENT [Switching to Elfabrio]
|
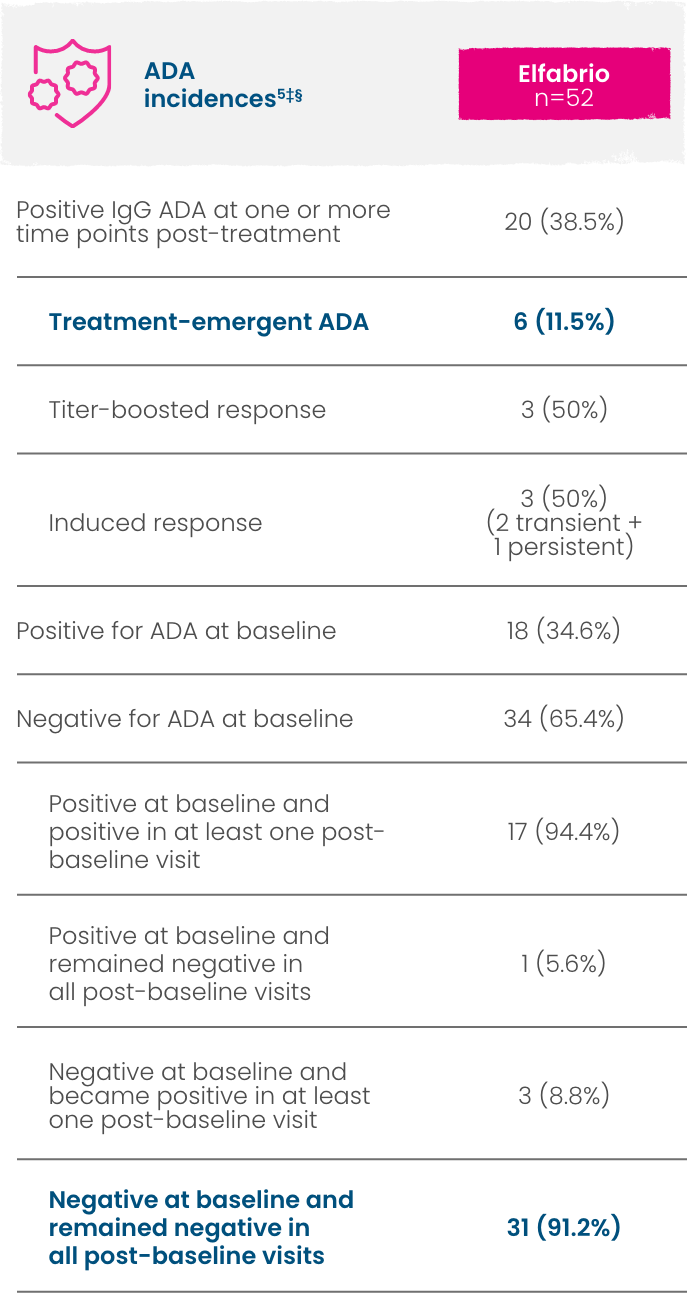
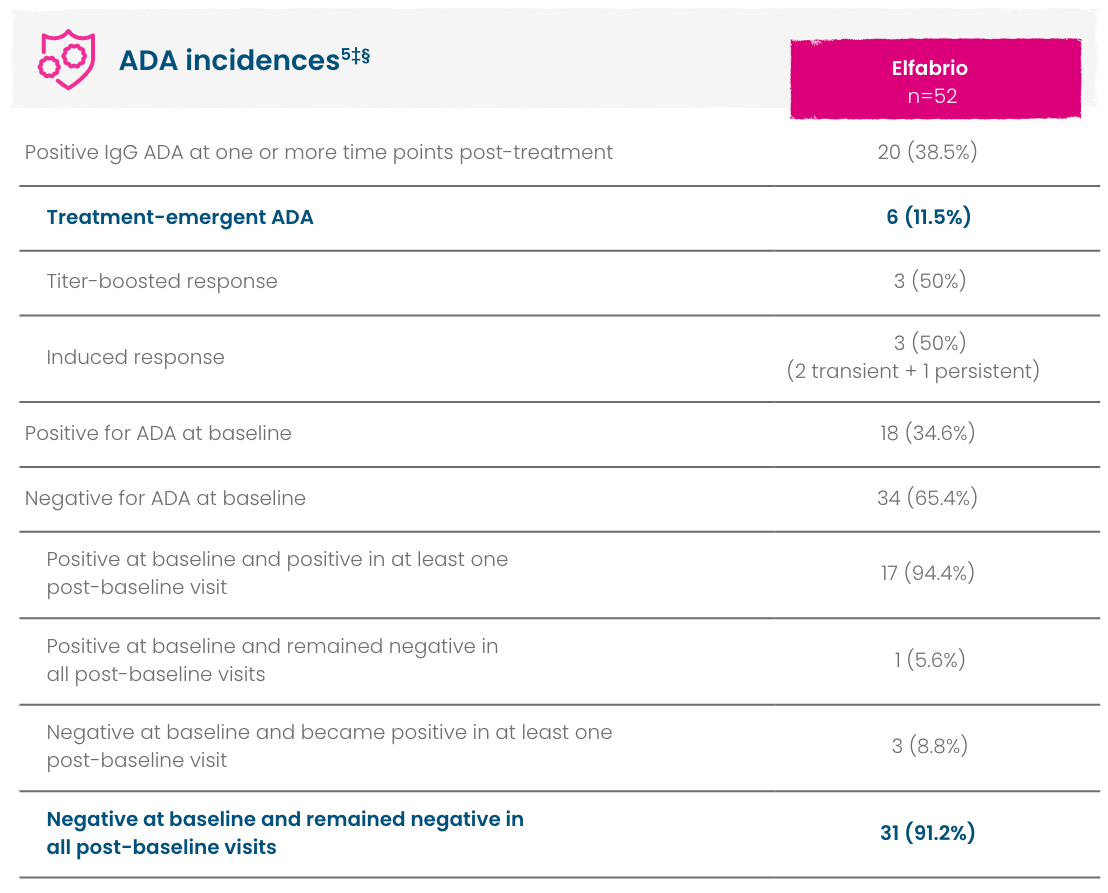
Picture this: Low immune response after switching to Elfabrio5
The efficacy and safety of Elfabrio, 1 mg/kg every 2 weeks, vs agalsidase beta were studied in BALANCE, a head-to-head, randomized, double-blind, 2-year, active-controlled study.1,3
| • |
Prior agalsidase beta: >1 year, average of 5.7 years
|
| • |
Primary study: 24 months (n=78, ITT=77, PP=72)
|
| • |
Open-label extension: Up to 60 months
|
Primary endpoint1,3
| • |
Annualized rate of change in eGFR (eGFR slope) assessed over 2 years
|
Safety endpoints3
| • |
Treatment-emergent adverse events, infusion-related reactions, anti-drug antibodies (ADAs)
|
BALANCE (Trial 2 in the Elfabrio Prescribing Information) provided confirmatory evidence in the FDA’s approval of Elfabrio. The data discussed are not intended to establish noninferiority or superiority to any other marketed drug product on the basis of safety or efficacy.5†
| † |
|
| eGFR, estimated glomerular filtration rate; FDA, Food and Drug Administration; ITT, intention to treat; PP, per protocol. |
| • |
Clinical significance of total ADAs and their effect on treatment is not completely understood
|
| • |
Testing for ADAs before treatment with Elfabrio and continuing to monitor routinely throughout treatment can give you the full picture
|
| ‡ |
The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. |
| § |
|
| IgG, immunoglobulin G. |
|
FRAGMENT [Starting Elfabrio]
|
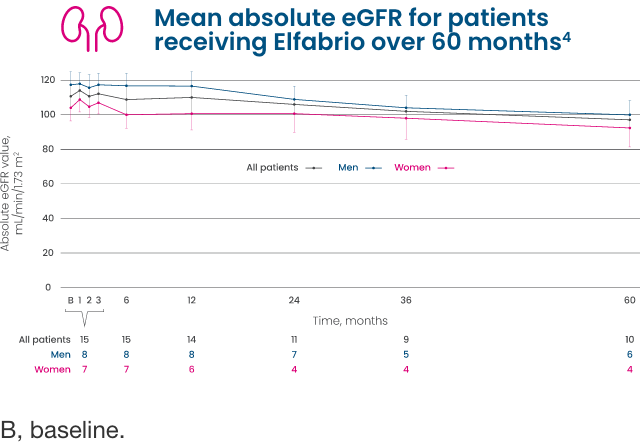
Treatment-naïve patients can start and stay with Elfabrio4
The safety and efficacy of Elfabrio were studied in a treatment-naïve patient population or patients not treated in the past 26 weeks in NAÏVE.1,4
Open-label | Safety study
| • |
Primary study: 3-month dose-ranging period (n=18)
|
| • |
Extension study: 9 months (n=16)
|
| • |
Open-label extension (1 mg/kg dose only; n=15): 60 months; up to 72 months of total treatment
|
Safety endpoints4,8
| • |
Treatment-emergent adverse events (TEAEs), infusion-related reactions, anti-drug antibodies (ADAs) |
Other endpoints4,8,9
| • |
Plasma lyso-Gb3, estimated glomerular filtration rate (eGFR), cardiac disease involvement, urine protein-to-creatinine ratio, pain |
|
Safety endpoints4,8
| • |
Treatment-emergent adverse events (TEAEs), infusion-related reactions, anti-drug antibodies (ADAs) |
|
Other endpoints4,8,9
| • |
Plasma lyso-Gb3, estimated glomerular filtration rate (eGFR), cardiac disease involvement, urine protein-to-creatinine ratio, pain |
|
|
Results at 1 year demonstrate:

|
Most adverse events were mild to moderate in treatment-naïve patients taking Elfabrio2
| • |
The most common related TEAEs were nausea (25%), chest discomfort, dizziness, rash, and fatigue (13% each)
|
| • |
4 severe TEAEs were reported, with migraine and anaphylaxis considered to be possibly related and definitely related to Elfabrio treatment, respectively. Anaphylaxis was IgE-mediated hypersensitivity-related bronchospasm that led to study withdrawal |
|

|
28.5% of Elfabrio-treated patients (4/14) who were ADA negative at baseline became ADA positive during Elfabrio treatment1†
|
| In the Elfabrio Prescribing Information, the NAÏVE study is referred to as Trial 1. |
| † |
The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. |
| IgE, immunoglobulin E; lyso-Gb3, globotriaosylsphingosine. |
Elfabrio helped to maintain renal function (eGFR) over 60 months4
|
FRAGMENT [Dosing and Administration]
|
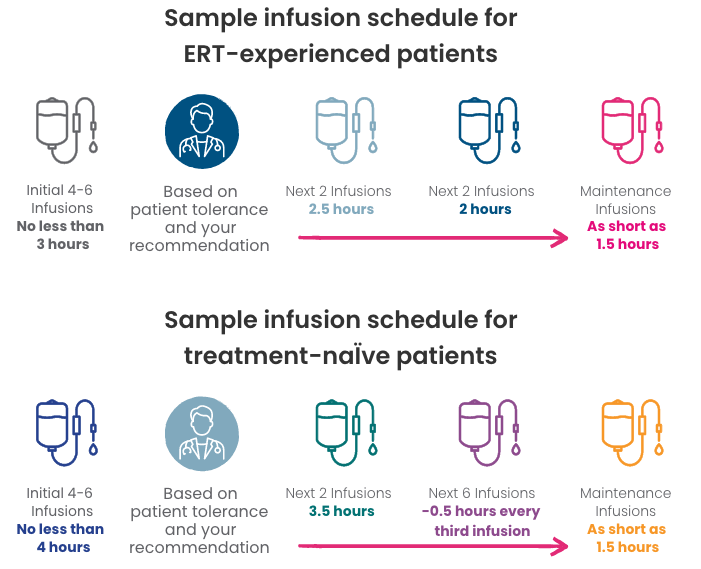
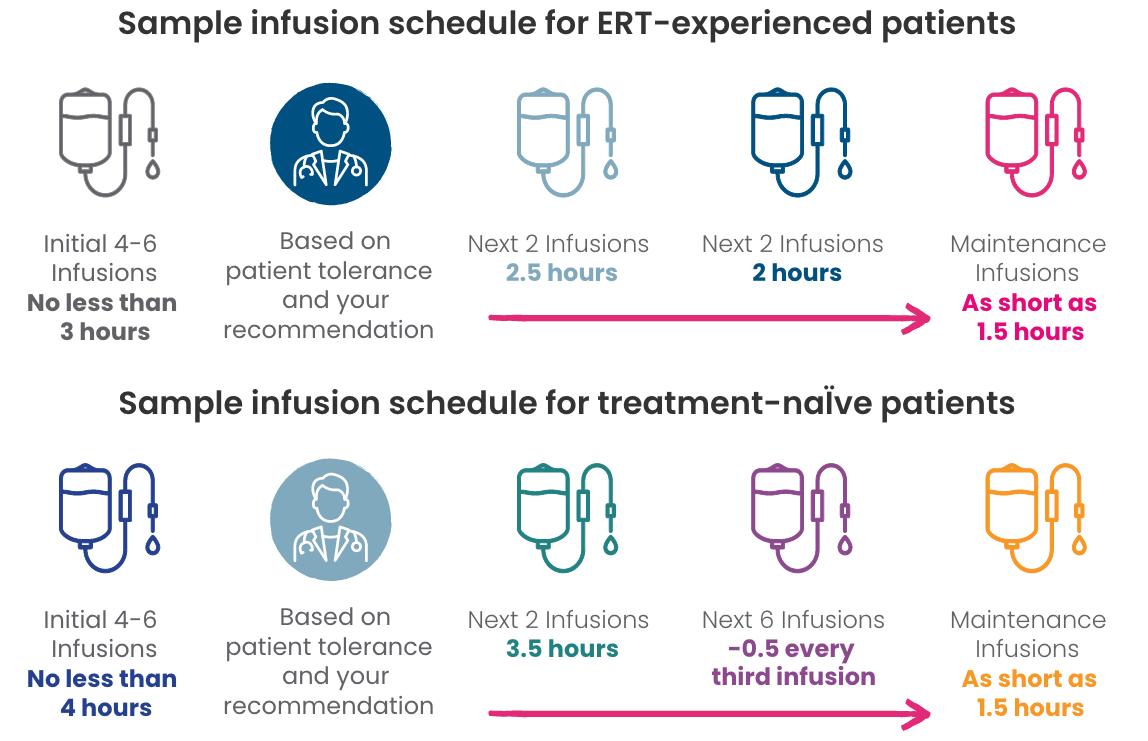
Dosing and administration designed with patients in mind1
| • |
Initial infusions (first 4-6 doses) take as little as 3 hours based on patient weight
|
| • |
If the patient is switching from a prior ERT with an infusion duration greater than 3 hours, start Elfabrio at the same infusion rate
|
| • |
Infusion duration may be decreased by 30 minutes after the initial infusions and at every third follow-up infusion to the minimum recommended duration of 1.5 hours
|
| • |
Consider whether tolerability has been established at each of these intervals and adjust the infusion rate at your discretion |
| † |
Patients receiving treatment or residing in MA or RI are not eligible for home infusion services. To receive home infusion support, patients must be referred to home infusion by their prescribing physician. Please see the full Terms and Conditions for additional eligibility requirements. |
|
FRAGMENT [Picture What's Possible]
|
Elfabrio: Picture what’s possible with the PEGylated ERT for Fabry disease1,2
Efficacy
Comparable mean change in estimated glomerular filtration rate (eGFR) observed vs agalsidase beta over 2 years1,5

Tolerability
Safety profile was assessed through long-term clinical trials including a head-to-head trial with an agalsidase beta control group1,3,4

Immunogenicity
Low rates of anti-drug antibody (ADA) formation with Elfabrio for naïve and treatment-experienced patients1,5†
|
|
|
Efficacy
Comparable mean change in estimated glomerular filtration rate (eGFR) observed vs agalsidase beta over 2 years1,5
|
|
|
Tolerability
Safety profile was assessed through long-term clinical trials including a head-to-head trial with an agalsidase beta control group1,3,4
|
|
|
Immunogenicity
Low rates of anti-drug antibody (ADA) formation with Elfabrio for naïve and treatment-experienced patients1,5†
|
|
| † |
The effect of IgG ADAs on the effectiveness of Elfabrio has not been fully characterized. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. |
| IgG, immunoglobulin G. |
|
|
Dedicated to helping you get patients started on Elfabrio
Insurance eligibility—Chiesi Total Care℠ assists you and your patients with:
|

Commercial insurance
If your patients have private insurance through their job or their own business
|

Government insurance
If your patients have Medicare, Medicaid, Veterans Affairs healthcare, or other government insurance
|

No insurance
If your patients have no insurance, they may be eligible for financial assistance
|
|
|
|
Commercial insurance
If your patients have private insurance through their job or their own business
|
|
|
Government insurance
If your patients have Medicare, Medicaid, Veterans Affairs healthcare, or other government insurance
|
|
|
No insurance
If your patients have no insurance, they may be eligible for financial assistance
|
|
Chiesi Total Care offers 2 copay programs for eligible patients:
|
Prescription copay
This covers the medication itself. Patients may pay as little as $0 for their Elfabrio prescription
|

Infusion program
This covers infusion supplies and administration (including home infusion). Patients may pay as little as $0 for these expenses
|
|
|
|
Prescription copay
This covers the medication itself. Patients may pay as little as $0 for their Elfabrio prescription
|
|
|
Infusion program
This covers infusion supplies and administration (including home infusion). Patients may pay as little as $0 for these expenses
|
|
To be eligible for these programs:
| • |
Patient must be enrolled in Chiesi Total Care. (Enrollment and Authorization Form will be mailed to your patient’s home)
|
| • |
Patient must have commercial insurance and a valid prescription for a US FDA-approved indication for Elfabrio
|
| • |
Patient must be a resident of the United States or one of its territories
|
Please see the full Terms and Conditions for additional eligibility requirements.
Government-funded plans are not eligible for patient support services that provide financial support through the programs. Patients receiving treatment or residing in MA or RI are not eligible for home infusion services. To receive home infusion support, patients must be referred to home infusion by their prescribing physician.
Let me know your availability for
{{customText [falsea calltruea video chattruean in-person meeting]}} in the next few weeks to discuss the difference Elfabrio could make for your Fabry patients. Please don’t hesitate to get in touch if you have any questions.
If you’d like to learn more about Elfabrio, please visit our website at elfabrio.com.
{{customText[falseSincerelytrueBest regardstrueI look forward to meeting with youtrueThank you]}},
{{UserName}}
{{UserEmailAddress}}
{{UserPhone}
|
 
|
Indication
Elfabrio® (pegunigalsidase alfa-iwxj) is indicated for the treatment of adults with confirmed Fabry disease.
Important Safety Information
WARNING: HYPERSENSITIVITY REACTIONS INCLUDING ANAPHYLAXIS
Patients treated with Elfabrio have experienced hypersensitivity reactions, including anaphylaxis. Appropriate medical support measures, including cardiopulmonary resuscitation equipment, should be readily available during Elfabrio administration. If a severe hypersensitivity reaction (eg, anaphylaxis) occurs, discontinue Elfabrio immediately and initiate appropriate medical treatment. In patients with severe hypersensitivity reaction, a desensitization procedure to Elfabrio may be considered.
|
Prior to Elfabrio administration, consider pretreating with antihistamines, antipyretics, and/or corticosteroids. Inform patients and caregivers of the signs and symptoms of hypersensitivity reactions and infusion-associated reactions (IARs), and instruct them to seek medical care immediately if such symptoms occur.
| • |
If a severe hypersensitivity reaction (including anaphylaxis) or severe IAR occurs, immediately discontinue Elfabrio administration and initiate appropriate medical treatment.
|
| • |
If a mild to moderate hypersensitivity reaction or IAR occurs, consider slowing the infusion rate or temporarily withholding the dose.
|
In clinical trials, 20 (14%) Elfabrio-treated patients experienced hypersensitivity reactions. Four Elfabrio-treated patients (3%) experienced anaphylaxis reactions that occurred within 5 to 40 minutes of the start of the initial infusion. The signs and symptoms of hypersensitivity reactions and anaphylaxis included headache, nausea, vomiting, throat tightness, facial and oral edema, truncal rash, tachycardia, hypotension, rigors, urticaria, intense pruritus, moderate upper airway obstructions, macroglossia, and mild lip edema.
In clinical trials, 41 (29%) Elfabrio-treated patients experienced one or more infusion-associated reactions, including hypersensitivity, nausea, chills, pruritus, rash, chest pain, dizziness, vomiting, asthenia, pain, sneezing, dyspnea, nasal congestion, throat irritation, abdominal pain, erythema, diarrhea, burning sensation, neuralgia, headache, paresthesia, tremor, agitation, increased body temperature, flushing, bradycardia, myalgia, hypertension, and hypotension.
A case of membranoproliferative glomerulonephritis with immune depositions in the kidney was reported during clinical trials. Monitor serum creatinine and urinary protein-to-creatinine ratio. If glomerulonephritis is suspected, discontinue treatment until a diagnostic evaluation can be conducted.
When switching to Elfabrio from a prior enzyme replacement therapy, the risk of hypersensitivity reactions and infusion-associated reactions may be increased in certain patients with pre-existing anti-drug antibodies (ADAs). Consider monitoring IgG and IgE ADAs and clinical or pharmacodynamic response (eg, plasma lyso-Gb3 levels).
The most common adverse reactions (≥15%) were infusion-associated reactions, nasopharyngitis, headache, diarrhea, fatigue, nausea, back pain, pain in extremity, and sinusitis.
Please see Full Prescribing Information for Elfabrio.
References: 1. Elfabrio. Prescribing Information. Chiesi Farmaceutici S.p.A.; 2023. 2. Schiffmann R, Goker-Alpan O, Holida M, et al. Pegunigalsidase alfa, a novel PEGylated enzyme replacement therapy for Fabry disease, provides sustained plasma concentrations and favorable pharmacodynamics: a 1-year phase 1/2 clinical trial. J Inherit Metab Dis. 2019;42(3):534-544. doi:10.1002/jimd.12080. 3. Wallace EL, Goker-Alpan O, Wilcox WR, et al. First results of a head-to-head trial of pegunigalsidase alfa vs agalsidase beta in Fabry disease: 2-year results of the phase 3 randomized, double-blind, BALANCE study. Poster presented at: WORLD Symposium: 19th Annual Research Meeting; February 22-26, 2023; Orlando, FL. https://protalixbiotherapeutics.gcs-web.com/static-files/58f1efe6-de3c-455d-b814-3e9e96373a8c. 4. Atta M, Hughes D, Gonzalez D, et al. Long-term safety and efficacy of pegunigalsidase alfa: a multicenter extension study in adult patients with Fabry disease. Poster presented at: 7th Update on Fabry Disease: Biomarkers, Progression and Treatment Opportunities in 2022; May 29-31, 2022; Würzburg, Germany. https://protalixbiotherapeutics.gcs-web.com/static-files/465d2891-4135-42e5-8581-f24e175cb07f. 5. US Food and Drug Administration. Drug approval package: Elfabrio; Multi-discipline Review. May 8, 2023. Accessed July 14, 2023. https://www.accessdata.fda.gov/drugsatfda_docs/nda/2023/761161Orig1s000MultidisciplineR.pdf. 6. Bernat J, Holida M, Longo N, et al. Long-term safety and efficacy of pegunigalsidase alfa administered every 4 weeks in patients with Fabry disease: 2-year interim results from the ongoing phase 3 BRIGHT51 open-label extension study. Poster presented at: WORLD Symposium: 19th Annual Research Meeting; February 22-26, 2023; Orlando, FL. https://protalixbiotherapeutics.gcs-web.com/static-files/d2dae305-1926-4418-9c62-3da527a62395. 7. West M, Linhart A, Dostalova G, et al. Switching from agalsidase alfa to pegunigalsidase alfa to treat patients with Fabry disease: 1 year of treatment data from BRIDGE, a phase 3 open-label study. Poster presented at: 7th Update on Fabry Disease: Biomarkers, Progression and Treatment Opportunities in 2022; May 29-31, 2022; Würzburg, Germany. https://protalixbiotherapeutics.gcs-web.com/static-files/e7e1cbc9-4858-42a2-b03f-1854e3e7a143. 8. Data on file. Chiesi Farmaceutici S.p.A.; December 2012. 9. Data on file. Chiesi Farmaceutici S.p.A.; January 2016.
|
|
|
|