|
||||||||||||||||||||||||

|

|
|||||||||||||||||||||||
|
Developed under the direction and sponsorship of Rigel Pharmaceuticals, Inc. |
||||||||||||||||||||||||
| Important Safety Information Full Prescribing Information Medication Guide | ||||||||||||||||||||||||
|
AFTER A VENETOCLAX-BASED REGIMEN, PATIENTS WITH AML MAY EXPERIENCE POOR OUTCOMES |
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
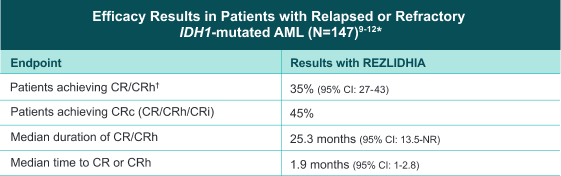
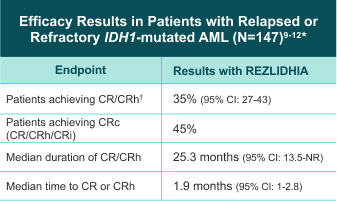
REZLIDHIA PROVIDED A CLINICALLY MEANINGFUL RESPONSE WITH DURABLE, COMPLETE REMISSION |
||||||||||||||||||||||||
|
REZLIDHIA is indicated for the treatment of adult patients with relapsed or refractory acute myeloid leukemia (AML) with a susceptible isocitrate dehydrogenase-1 (IDH1) mutation as detected by an FDA-approved test. |
||||||||||||||||||||||||
|
SELECT IMPORTANT SAFETY INFORMATION |
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
Please see additional Important Safety Information below and Full Prescribing Information, including Boxed WARNING. |
||||||||||||||||||||||||
|
|
|||||||||||||||||||||||
|
View the efficacy of REZLIDHIA from the pivotal trial and long-term analysis. |
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
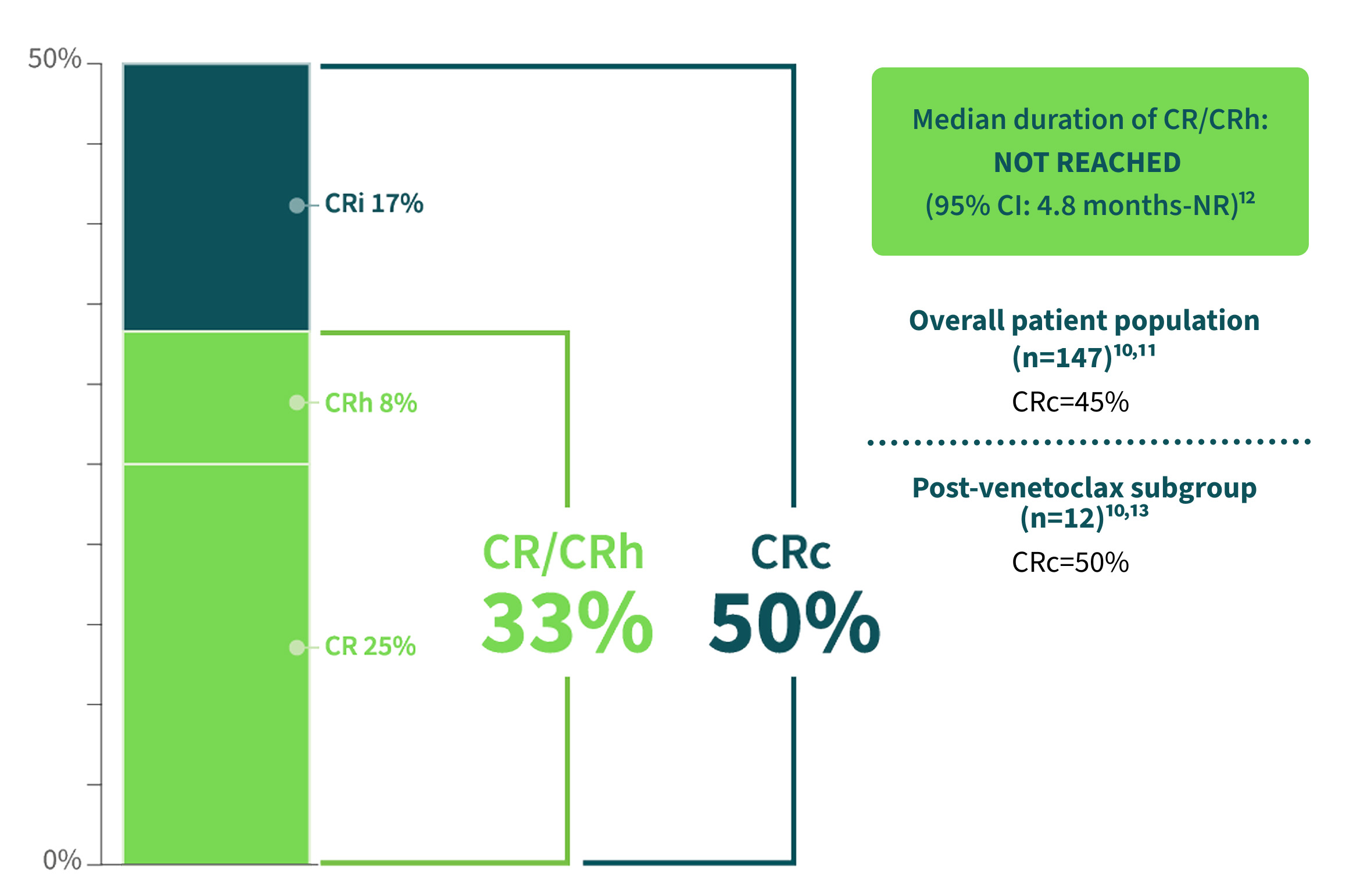
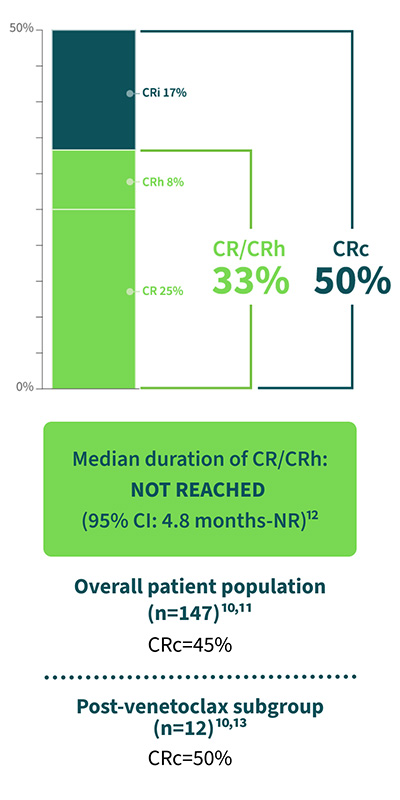
PATIENTS TREATED WITH VENETOCLAX IN THE PIVOTAL TRIAL HAD RESPONSES THAT WERE CONSISTENT WITH THE OVERALL POPULATION |
||||||||||||||||||||||||
|
Findings from a subgroup analysis of 12 patients treated with a venetoclax-based regimen prior to treatment with REZLIDHIA.10,11 |
||||||||||||||||||||||||
|
Clinical Response Rates (n=12)13 |
||||||||||||||||||||||||
|
|
|||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
For patients with mIDH1 AML who relapse or are refractory to initial treatment, choose REZLIDHIA as the first R/R targeted therapy. |
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
IMPORTANT SAFETY INFORMATION (CONT'D) WARNINGS AND PRECAUTIONS Differentiation Syndrome REZLIDHIA can cause differentiation syndrome. In the clinical trial of REZLIDHIA in patients with relapsed or refractory AML, differentiation syndrome occurred in 16% of patients, with grade 3 or 4 differentiation syndrome occurring in 8% of patients treated, and fatalities in 1% of patients. Differentiation syndrome is associated with rapid proliferation and differentiation of myeloid cells and may be life-threatening or fatal. Symptoms of differentiation syndrome in patients treated with REZLIDHIA included leukocytosis, dyspnea, pulmonary infiltrates/pleuropericardial effusion, kidney injury, fever, edema, pyrexia, and weight gain. Of the 25 patients who experienced differentiation syndrome, 19 (76%) recovered after treatment or after dose interruption of REZLIDHIA. Differentiation syndrome occurred as early as 1 day and up to 18 months after REZLIDHIA initiation and has been observed with or without concomitant leukocytosis. If differentiation syndrome is suspected, temporarily withhold REZLIDHIA and initiate systemic corticosteroids (e.g., dexamethasone 10 mg IV every 12 hours) for a minimum of 3 days and until resolution of signs and symptoms. If concomitant leukocytosis is observed, initiate treatment with hydroxyurea, as clinically indicated. Taper corticosteroids and hydroxyurea after resolution of symptoms. Differentiation syndrome may recur with premature discontinuation of corticosteroids and/or hydroxyurea treatment. Institute supportive measures and hemodynamic monitoring until improvement; withhold dose of REZLIDHIA and consider dose reduction based on recurrence. Hepatotoxicity REZLIDHIA can cause hepatotoxicity, presenting as increased alanine aminotransferase (ALT), increased aspartate aminotransferase (AST), increased blood alkaline phosphatase, and/or elevated bilirubin. Of 153 patients with relapsed or refractory AML who received REZLIDHIA, hepatotoxicity occurred in 23% of patients; 13% experienced grade 3 or 4 hepatotoxicity. One patient treated with REZLIDHIA in combination with azacitidine in the clinical trial, a combination for which REZLIDHIA is not indicated, died from complications of drug-induced liver injury. The median time to onset of hepatotoxicity in patients with relapsed or refractory AML treated with REZLIDHIA was 1.2 months (range: 1 day to 17.5 months) after REZLIDHIA initiation, and the median time to resolution was 12 days (range: 1 day to 17 months). The most common hepatotoxicities were elevations of ALT, AST, blood alkaline phosphatase, and blood bilirubin. Monitor patients frequently for clinical symptoms of hepatic dysfunction such as fatigue, anorexia, right upper abdominal discomfort, dark urine, or jaundice. Obtain baseline liver function tests prior to initiation of REZLIDHIA, at least once weekly for the first two months, once every other week for the third month, once in the fourth month, and once every other month for the duration of therapy. If hepatic dysfunction occurs, withhold, reduce, or permanently discontinue REZLIDHIA based on recurrence/severity. ADVERSE REACTIONS The most common (≥20%) adverse reactions, including laboratory abnormalities, were aspartate aminotransferase increased, alanine aminotransferase increased, potassium decreased, sodium decreased, alkaline phosphatase increased, nausea, creatinine increased, fatigue/malaise, arthralgia, constipation, lymphocytes increased, bilirubin increased, leukocytosis, uric acid increased, dyspnea, pyrexia, rash, lipase increased, mucositis, diarrhea and transaminitis. DRUG INTERACTIONS
LACTATION Advise women not to breastfeed during treatment with REZLIDHIA and for 2 weeks after the last dose. GERIATRIC USE No overall differences in effectiveness were observed between patients 65 years and older and younger patients. Compared to patients younger than 65 years of age, an increase in incidence of hepatotoxicity and hypertension was observed in patients ≥65 years of age. HEPATIC IMPAIRMENT In patients with mild or moderate hepatic impairment, closely monitor for increased probability of differentiation syndrome. Please see REZLIDHIAhcp.com for Full Prescribing Information, including Boxed WARNING. REFERENCES: 1. Bewersdorf JP, Shallis RM, Derkach A, et al. Efficacy of FLT3 and IDH1/2 inhibitors in patients with acute myeloid leukemia previously treated with venetoclax. Leuk Res. 2022;122:106942. doi:10.1016/j.leukres.2022.106942 2. Abaza Y, Winer ES, Murthy GSG, et al. Clinical outcomes of hypomethylating agents plus venetoclax as frontline treatment in patients 75 years and older with acute myeloid leukemia: real-world data from eight US academic centers. Am J Hematol. Published online February 11, 2024. doi:10.1002/ajh.27231 3. Thol F, Döhner H, Ganser A. How I treat refractory and relapsed acute myeloid leukemia. Blood. 2024;143(1):11-20. doi:10.1182/blood.2023022481 4. Gangat N, Ilyas R, Johnson IM, et al. Outcome of patients with acute myeloid leukemia following failure of frontline venetoclax plus hypomethylating agent therapy. Haematologica. 2023;108(11):3170-3174. doi:10.3324/haematol.2022.282677 5. Khanna V, Azenkot T, Liu SQ, et al. Outcomes with molecularly targeted agents as salvage therapy following frontline venetoclax + hypomethylating agent in adults with acute myeloid leukemia: a multicenter retrospective analysis. Leuk Res. 2023;131:107331. doi:10.1016/j.leukres.2023.107331 6. Maiti A, Qiao W, Sasaki K, et al. Venetoclax with decitabine vs intensive chemotherapy in acute myeloid leukemia: a propensity score matched analysis stratified by risk of treatment-related mortality. Am J Hematol. 2021;96(3):282-291. doi:10.1002/ajh.26061 7. Tenold ME, Moskoff BN, Benjamin DJ, et al. Outcomes of adults with relapsed/refractory acute myeloid leukemia treated with venetoclax plus hypomethylating agents at a comprehensive cancer center. Front Oncol. 2021;11:649209. doi:10.3389/fonc.2021.649209 8. Cortes J, Jonas BA, Schiller G, et al. Olutasidenib in post-venetoclax patients with mutant isocitrate dehydrogenase 1 (mIDH1) acute myeloid leukemia (AML). Leuk Lymphoma. Published online March 27, 2024. doi:10.1080/10428194.2024.2333451 9. REZLIDHIA®. Package insert. Rigel Pharmaceuticals, Inc; 2022. 10. de Botton S, Fenaux P, Yee K, et al. Olutasidenib (FT-2102) induces durable complete remissions in patients with relapsed or refractory IDH1-mutated AML. Blood Adv. 2023;7(13):3117-3127. doi:10.1182/bloodadvances.2022009411 11. Cortes J, Curti A, Fenaux P, et al. Olutasidenib for mutated IDH1 acute myeloid leukemia: final five-year results from the phase 2 pivotal cohort. J Hematol Oncol. 2025;18(1):102. doi:10.1186/s13045-025-01751-w 12. Data on file, Rigel Pharmaceuticals, Inc. January 2025. 13. Cortes J, Curti A, Fenaux P, et al. Olutasidenib for mutated IDH1 acute myeloid leukemia: final five-year results from the phase 2 pivotal cohort (supplemental data). J Hematol Oncol. 2025; https://link.springer.com/article/10.1186/s13045-025-01751-w#Sec20 |
||||||||||||||||||||||||
|
|
||||||||||||||||||||||||
|
© 2026 Rigel Pharmaceuticals, Inc. All rights reserved. REZ_AML-25092 0226 |
||||||||||||||||||||||||
|
Help |
||||||||||||||||||||||||