|
|
||||||||||
|
|
||||||||||
|
STRONG, SUSTAINED RESULTS GAVRETO is the only once-daily therapy designed to |
||||||||||
|
|
||||||||||
| [Variable salutation: false Hello true Hi true Dear true Good morning true Good afternoon] [Variable title: false true Dr. true Nurse true Mr. true Mrs. true Ms.] [Variable/optional name: false First Name true Last Name true First Name Last Name] | ||||||||||
[Variable opening message]
|
||||||||||
|
INDICATION
SELECT SAFETY INFORMATION Please see additional Important Safety Information below and full Prescribing Information. |
||||||||||
|
||||||||||
|
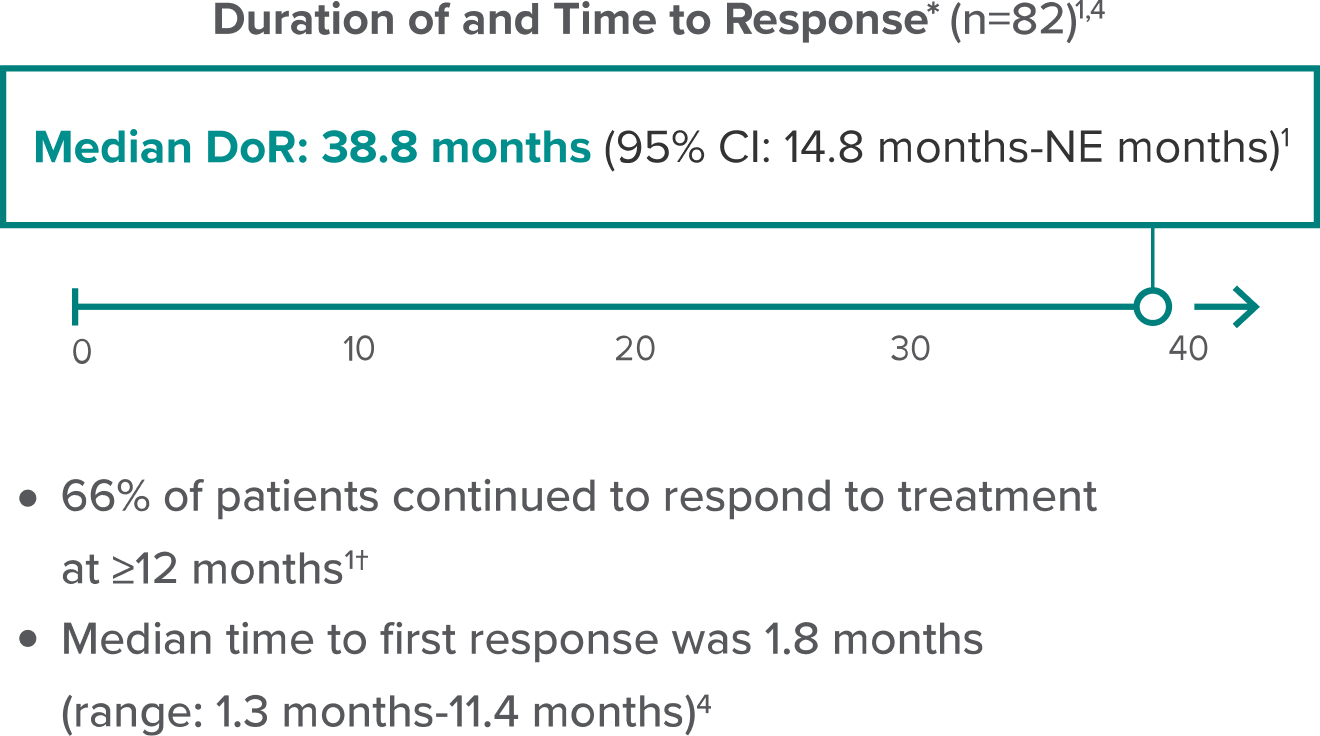
GAVRETO was studied in patient populations representative of those seen in the real world1,2 Efficacy and safety with GAVRETO (400 mg orally once daily) were evaluated in patients with RET fusion+ mNSCLC in the ARROW study, a phase 1/2, nonrandomized, open-label, single-arm, multicohort, multicenter clinical trial. Patients with asymptomatic CNS metastases, including patients with stable or decreasing steroid use within 2 weeks prior to study entry, were enrolled.1,3 GAVRETO demonstrated substantial response in previously platinum-treated patients1
|
||||||||||
|
||||||||||
|
||||||||||
|
||||||||||
[Variable closing message]
|
||||||||||
| [Variable sign-off: false Sincerely true Kind regards true Best true Talk soon true Thank you true Thanks again], | ||||||||||
[Prepopulated representative phone number] [Prepopulated representative email] |
||||||||||
|
SELECT SAFETY INFORMATION Hepatotoxicity: Serious hepatic adverse reactions occurred in 1.5% of patients treated with GAVRETO. Increased aspartate aminotransferase (AST) occurred in 49% of patients, including Grade 3 or 4 in 7% and increased alanine aminotransferase (ALT) occurred in 37% of patients, including Grade 3 or 4 in 4.8%. The median time to first onset for increased AST was 15 days (range: 5 days to 2.5 years) and increased ALT was 24 days (range: 7 days to 3.7 years). Monitor AST and ALT prior to initiating GAVRETO, every 2 weeks during the first 3 months, then monthly thereafter and as clinically indicated. Withhold, reduce dose or permanently discontinue GAVRETO based on severity. Hemorrhagic Events: Serious, including fatal, hemorrhagic events can occur with GAVRETO. Grade ≥3 events occurred in 4.1% of patients treated with GAVRETO including one patient with a fatal hemorrhagic event. Permanently discontinue GAVRETO in patients with severe or life-threatening hemorrhage. Tumor Lysis Syndrome (TLS): Cases of TLS have been reported in patients with medullary thyroid carcinoma receiving GAVRETO. Patients may be at risk of TLS if they have rapidly growing tumors, a high tumor burden, renal dysfunction, or dehydration. Closely monitor patients at risk, consider appropriate prophylaxis including hydration, and treat as clinically indicated. Risk of Impaired Wound Healing: Impaired wound healing can occur in patients who receive drugs that inhibit the vascular endothelial growth factor (VEGF) signaling pathway. Therefore, GAVRETO has the potential to adversely affect wound healing. Withhold GAVRETO for at least 5 days prior to elective surgery. Do not administer for at least 2 weeks following major surgery and until adequate wound healing. The safety of resumption of GAVRETO after resolution of wound healing complications has not been established. Embryo-Fetal Toxicity: Based on findings from animal studies and its mechanism of action, GAVRETO can cause fetal harm when administered to a pregnant woman. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective non-hormonal contraception during treatment with GAVRETO and for 2 weeks after the last dose. Advise males with female partners of reproductive potential to use effective contraception during treatment with GAVRETO and for 1 week after the last dose. Common adverse reactions (≥25%) were musculoskeletal pain, constipation, hypertension, diarrhea, fatigue, edema, pyrexia, and cough. Common Grade 3/4 laboratory abnormalities (≥2%) were decreased lymphocytes, decreased neutrophils, decreased hemoglobin, decreased phosphate, decreased leukocytes, decreased sodium, increased aspartate aminotransferase (AST), increased alanine aminotransferase (ALT), decreased calcium (corrected), decreased platelets, increased alkaline phosphatase, increased potassium, decreased potassium, and increased bilirubin. Avoid coadministration of GAVRETO with strong or moderate CYP3A inhibitors, P-gp inhibitors, or combined P-gp and strong or moderate CYP3A inhibitors. If coadministration cannot be avoided, reduce the GAVRETO dose. Avoid coadministration of GAVRETO with strong or moderate CYP3A inducers. If coadministration cannot be avoided, increase the GAVRETO dose. Lactation: Advise women not to breastfeed during treatment with GAVRETO and for 1 week after the last dose. Pediatric Use: Monitor open growth plates in adolescent patients. Consider interrupting or discontinuing GAVRETO if abnormalities occur. You may report side effects to the FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. Please click here to see full Prescribing Information and Patient Information for GAVRETO. References: 1. GAVRETO® [Package insert], South San Francisco, CA: Rigel Pharmaceuticals, Inc. 2. Hess LM, Han Y, Zhu YE, Bhandari NR, Sireci A. Characteristics and outcomes of patients with RET-fusion positive non-small lung cancer in real-world practice in the United States. BMC Cancer. 2021;21(1):28. 3. Phase 1/2 study of the highly-selective RET inhibitor, pralsetinib (BLU-667), in participants with thyroid cancer, non-small cell lung cancer, and other advanced solid tumors (ARROW). ClinicalTrials.gov identifier: NCT03037385. https://clinicaltrials.gov/ct2/show/NCT03037385. Accessed January 15, 2025. 4. GAVRETO: Data on file, Rigel Pharmaceuticals, Inc. December 2024. 5. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Non-Small Cell Lung Cancer V.3.2025. © National Comprehensive Cancer Network, Inc. 2025. All rights reserved. Accessed January 15, 2025. To view the most recent and complete version of the guideline, go online to NCCN.org. |
||||||||||
|