|
If there are problems with how this message is displayed, click here to view it in a web browser.
|
If there are problems with how this message is displayed, click here to view it in a web browser.
|
|
|
utility-head-001
|
|
utility-head-002
|
|
utility-greet-001
|
Dear [Title][First Name][Last Name], [Designation],
|
|
|
hero-gen-001
Switch on
XCOPRI sooner
|
A chance at zero seizures
can’t wait.
|

|
|
Switch on
XCOPRI sooner
|
A chance at zero seizures
can’t wait.
|
|
|
|
|
|
|
|
hero-gen-002
|
Help light the way
forward with the
power of once-daily
XCOPRI1
|

|
|
A chance at zero seizures
can’t wait.
|
|
|
Help light the way
forward with the
power of once-daily
XCOPRI1
|
|
A chance at zero seizures
can’t wait.
|
|
|
|
|
ref-hero-gen-002
|
Reference for section "Help light the way forward...," 1. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc.
|
|
|
hero-urg-001
|
Uncontrolled seizures continue to be a reality for many patients1
|
|
The consequences of seizures—physical, emotional, and cognitive—can take their toll on patients’ daily lives.
|
|
|


|
|
|
|
ref-hero-urg-001
|
Reference for section “Uncontrolled seizures continue...”: 1. Josephson CB, Patten SB, Bulloch A, et al. The impact of seizures on epilepsy outcomes: a national, community-based survey. Epilepsia. 2017;58(5):764-771.
|
|
|
hero-moa-001
|
2 mechanisms, 1 treatment1-5
|
|
XCOPRI reduces neuronal excitability through a unique dual MOA
|
|
|
|
|
ref-hero-moa-001
|
References for section “2 mechanisms, 1 treatment”: 1. Guignet M, Campbell A, White HS. Cenobamate (XCOPRI): Can preclinical and clinical evidence provide insight into its mechanism of action? Epilepsia. 2020;61(11):2329-2339. 2. Perucca E, Bialer M, White HS. New GABA-targeting therapies for the treatment of seizures and epilepsy: I. role of GABA as a modulator of seizure activity and recently approved medications acting on the GABA system. CNS Drugs. 2023;37(9):755-779. 3. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc. 4. Sharma R, Nakamura M, Neupane C, et al. Positive allosteric modulation of GABAA receptors by a novel antiepileptic drug cenobamate. Eur J Pharmacol. 2020;879:173117. 5. Nakamura M, Cho JH, Shin H, Jang IS. Effects of cenobamate (YKP3089), a newly developed anti-epileptic drug, on voltage-gated sodium channels in rat hippocampal CA3 neurons. Eur J Pharmacol. 2019;855:175-182.
|
|
|
hero-eff-001
|
Why switch on XCOPRI sooner?
|
|
Because a chance at zero seizures can’t wait.
|
|
|
|
|
hero-saf-001
|
Explore the safety profile of XCOPRI
|
|
XCOPRI offers well-studied safety, with 5-year retention data.1,2
|
|
|
|
|
ref-hero-saf-001
|
References for section “Explore the safety profile": 1. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc. 2. Sander JW, Rosenfeld WE, Halford JJ, Steinhoff BJ, Biton V, Toledo M. Long-term individual retention with cenobamate in adults with focal seizures: pooled data from the clinical development program. Epilepsia. 2022;63(1):139-149.
|
|
|
hero-tol-001
|
Help light the way forward with XCOPRI
|
|
Consider the branded ASM epileptologists prescribe most.*
|
| * |
By NBRx, as of July 2025. |
|
ASM=anti-seizure medication. |
|
|
|
|
|
hero-acc-001
|
Getting patients access to XCOPRI
|
|
Discover how we’re helping you switch on XCOPRI for your patients.
|
|
|
|
|
hero-dos-001
|
Convenient once-daily dosing1
|
|
|
|
XCOPRI offers a personalized treatment approach for your patients.
|
|
|
|
ref-hero-dos-001
|
Reference for section “Convenient once-daily dosing”: 1. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc.
|
|
|
body-urg-001
|
Patients have a lot to lose with just 1 seizure
|
|
When seizures remain uncontrolled, patients are1*:
|
| ~6x |
| more likely to have depression |
|
|
| 4.5x |
| more likely to be prevented from driving |
|
|
| 3x |
| more likely to experience limitations in employment |
|
|
| 2x |
| more likely to have limits in education |
|
|
|
|
Patients have a lot to lose with just 1 seizure
|
|
When seizures remain uncontrolled, patients are1*:
|
| ~6x |
more likely
to have
depression
|
|
|
| 4.5x |
more likely to
be prevented
from driving
|
|
|
| 3x |
more likely to
experience
limitations in
employment
|
|
|
| 2x |
more likely to
have limits
in education
|
|
|
|
|
|


|
| Patients with seizures have an increased risk of SUDEP2† |
| Up to 9.3 deaths per 1000 person-years in patients with refractory epilepsy3 |
|
| Secondary generalized tonic-clonic seizures put patients at a 30x higher risk for SUDEP compared to other seizure types4 |
|
| Up to 9.3 deaths per 1000 person-years in patients with refractory epilepsy3 |
Secondary generalized tonic-clonic seizures put patients at a 30x higher risk for SUDEP compared to other seizure types4 |
|
|
|
| * |
Based on data that compared patients who had ≥1 seizure in the past 5 years with those who experienced no seizures in the past 5 years. |
| † |
Based on data that compared patients who had ≥1 seizure in the previous year with those who had zero seizures in the previous year. |
|
SUDEP=sudden unexpected death in epilepsy. |
|
|
|
|
ref-body-urg-001
|
References for section “Patients have a lot to lose...”: 1. Josephson CB, Patten SB, Bulloch A, et al. The impact of seizures on epilepsy outcomes: a national, community-based survey. Epilepsia. 2017;58(5):764-771. 2. Nilsson L, Farahmand BY, Persson P-G, Thiblin I, Tomson T. Risk factors for sudden unexpected death in epilepsy: a case-control study. Lancet. 1999;353(9156):888-893. 3. Devinsky O, Hesdorffer DC, Thurman DJ, Lhatoo S, Richerson G. Sudden unexpected death in epilepsy: epidemiology, mechanisms, and prevention. Lancet Neurol. 2016;15(10):1075-1088. 4. Shlobin NA, Thijs RD, Benditt DG, Zeppenfeld K, Sander JW. Sudden death in epilepsy: the overlap between cardiac and neurological factors. Brain Commun. 2024;6(5):fcae309.
|
|
|
body-urg-002
| Many patients have a history of being let down |
| During the past 3 decades, despite new ASMs coming to market, seizure freedom rates have remained nearly the same.1,2* |
| Rates of zero seizures by decade of approval for a range of ASMs3† |
|
|
| 1990-1999 |
| 2.1%-8.7% |
| vs 0%-2.2% with placebo4,5 |
| 2000-2009 |
| 2.2%-7.4% |
| vs 0.8%-1.2% with placebo6,7 |
| 2010-2019 |
| 2.0%-8.2% |
| vs 0%-2% with placebo8-10 |
|
| 1990-1999 |
| 2.1%-8.7% |
| vs 0%-2.2% with placebo4,5 |
|
| 2000-2009 |
| 2.2%-7.4% |
| vs 0.8%-1.2% with placebo6,7 |
|
| 2010-2019 |
| 2.0%-8.2% |
| vs 0%-2% with placebo8-10 |
|
|
|
|
| Prior to the 1990s, there was little information on seizure freedom rates with ASMs used as add-on therapy—and even less information about how these rates were determined.3 |
|
| * |
Seizure freedom was defined as a patient experiencing no seizures for the previous 12 months or longer.1 |
| † |
Data from pivotal trials. |
|
ASMs=anti-seizure medications. |
|
|
|
|
ref-body-urg-002
|
References for section “Many patients have a history of being let down”: 1. Chen Z, Brodie MJ, Liew D, Kwan P. Treatment outcomes in patients with newly diagnosed epilepsy treated with established and new antiepileptic drugs: a 30-year longitudinal cohort study. JAMA Neurol. 2018;75(3):279-286. 2. Chen Z, Brodie MJ, Liew D, Kwan P. Treatment outcomes in patients with newly diagnosed epilepsy treated with established and new antiepileptic drugs: a 30-year longitudinal cohort study. JAMA Neurol. 2018;75(3)(suppl):1-14. 3. Halford JJ, Edwards JC. Seizure freedom as an outcome in epilepsy treatment clinical trials. Acta Neurol Scand. 2020;142(2):91-107. 4. Keppra [package insert]. Smyrna, GA: UCB, Inc; 2024. 5. Topamax [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2025. 6. Vimpat [package insert]. Smyrna, GA: UCB, Inc; 2023. 7. Sabril [package insert]. Deerfield, IL: Lundbeck; 2021. 8. Fycompa [package insert]. Woodcliff Lake, NJ: Eisai Inc; 2023. 9. Aptiom [package insert]. Marlborough, MA: Sunovion Pharmaceuticals, Inc; 2019. 10. Potiga [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2024.
|
|
|
body-urg-003
|
|
| Patients with seizures have an increased risk of SUDEP1* |
| Up to 9.3 deaths per 1000 person-years in patients with refractory epilepsy2 |
|
| Secondary generalized tonic-clonic seizures put patients at a 30x higher risk for SUDEP compared to other seizure types3 |
|
| Up to 9.3 deaths per 1000 person-years in patients with refractory epilepsy2 |
Secondary generalized tonic-clonic seizures put patients at a 30x higher risk for SUDEP compared to other seizure types3 |
|
|
| * |
Based on data that compared patients who had ≥1 seizure in the previous year with those who had zero seizures in the previous year. |
|
SUDEP=sudden unexpected death in epilepsy. |
|
|
|
|
ref-body-urg-003
|
References for section "Patients with seizures have an increased risk of SUDEP": 1. Nilsson L, Farahmand BY, Persson P-G, Thiblin I, Tomson T. Risk factors for sudden unexpected death in epilepsy: a case-control study. Lancet. 1999;353(9156):888-893. 2. Devinsky O, Hesdorffer DC, Thurman DJ, Lhatoo S, Richerson G. Sudden unexpected death in epilepsy: epidemiology, mechanisms, and prevention. Lancet Neurol. 2016;15(10):1075-1088. 3. Shlobin NA, Thijs RD, Benditt DG, Zeppenfeld K, Sander JW. Sudden death in epilepsy: the overlap between cardiac and neurological factors. Brain Commun. 2024;6(5):fcae309.
|
|
|
body-urg-004
| Patients with uncontrolled seizures have an increased risk of comorbidities1*† |
 |
Cardiac and
Metabolic |
| 1.5-2x |
more likely to have atrial fibrillation (AFib) |
|
 |
Neuro-psychiatric |
| 3x |
more likely to have non-epileptic seizures |
|
 |
Neurologic |
| 1.5-2x |
more likely to have brain trauma |
| 1.5-2x |
more likely to develop dementia/Alzheimer’s |
| 1.5-2x |
more likely to have a stroke |
|
|
Cardiac and
Metabolic |
|
1.5-2x |
more likely to have atrial fibrillation (AFib) |
|
|
Neuro-psychiatric |
|
3x |
more likely to have non-epileptic seizures |
|
|
Neurologic |
|
| 1.5-2x |
more likely to have brain trauma |
| 1.5-2x |
more likely to develop dementia/Alzheimer’s |
| 1.5-2x |
more likely to have a stroke |
|
|
|
| * |
Incidence of comorbidities in patients with uncontrolled vs controlled epilepsy following initiation of first-line and third-line ASM. |
| † |
Uncontrolled epilepsy was defined by ≥1 of the following events: seizure-related inpatient visit, seizure-related emergency room visit, or new ASM line of therapy initiation. |
|
ASM=anti-seizure medication. |
|
|
|
|
ref-body-urg-004
|
Reference for section “Patients with uncontrolled seizures have an increased risk of comorbidities”: 1. Faught E, Kerr WT, Stern S, Wade CT, Klatte E. Increased incidence of comorbidities in patients with uncontrolled epilepsy. Poster presented at: American Epilepsy Society Annual Meeting; December 1-3, 2023; Orlando, FL.
|
|
|
body-eff-001
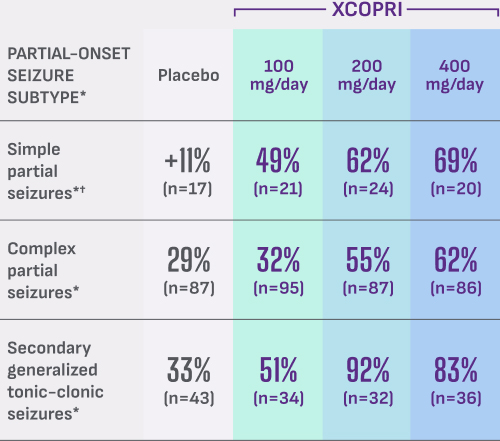
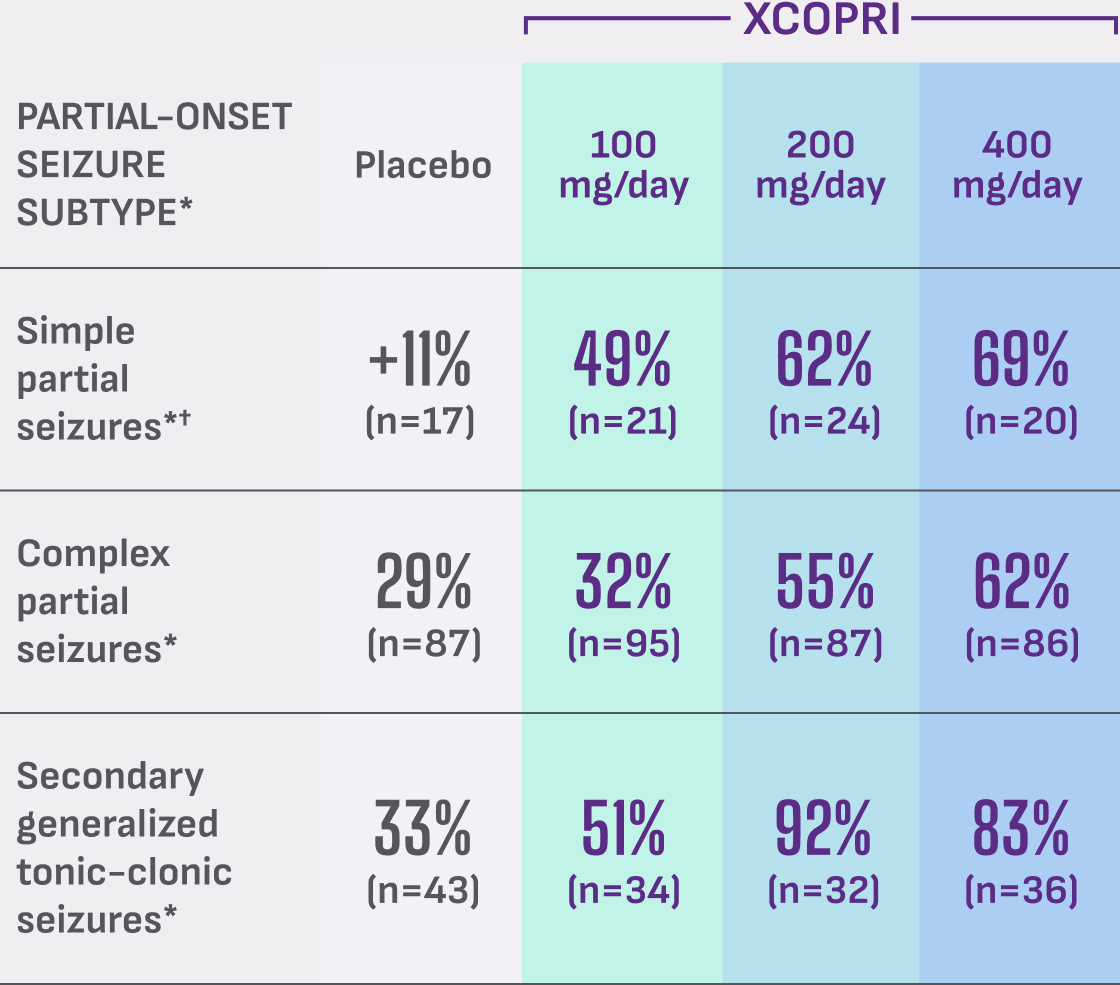
| Powerful reduction across multiple seizure types |
| Results from a study of patients with a median of 9 seizures/28 days at baseline1,2 |
| Additional secondary outcome: |
| Median percentage reduction in 28-day seizure frequency in partial-onset seizure subtypes |
| (12-week maintenance phase)1,3 |
|
|
See full study design and population 
|
See full study design and population
|
| * |
Partial-onset=focal; simple partial=focal aware; complex partial=focal unaware; secondary generalized tonic-clonic=focal to bilateral tonic-clonic.4 |
| † |
Only patients with simple partial motor seizures were included in the study. |
|
|
|
|
ref-body-eff-001
|
References for section "Powerful reduction across multiple seizure types": 1. Krauss GL, Klein P, Brandt C, et al. Safety and efficacy of adjunctive cenobamate (YKP3089) in patients with uncontrolled focal seizures: a multicentre, double-blind, randomised, placebo-controlled, dose-response trial. Lancet Neurol. 2020;19(1):38-48. 2. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc. 3. Krauss GL, Klein P, Brandt C, et al. Safety and efficacy of adjunctive cenobamate (YKP3089) in patients with uncontrolled focal seizures: a multicentre, double-blind, randomised, placebo-controlled, dose-response trial. Lancet Neurol. 2020;19(1)(suppl 1):S1-S7. 4. Fisher RS, Cross JH, French JA, et al. Operational classification of seizure types by the International League Against Epilepsy: position paper of the ILAE Commission for Classification and Terminology. Epilepsia. 2017;58(4):522-530.
|
|
|
body-eff-002
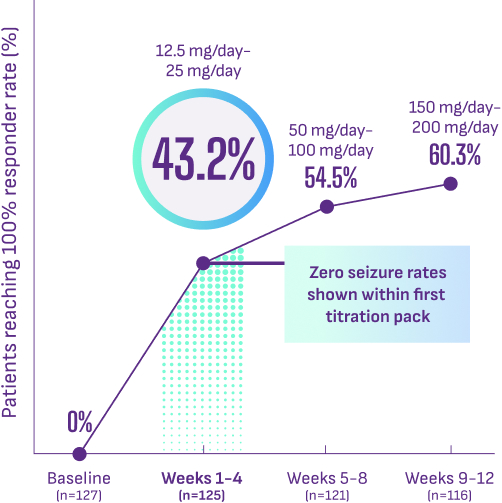
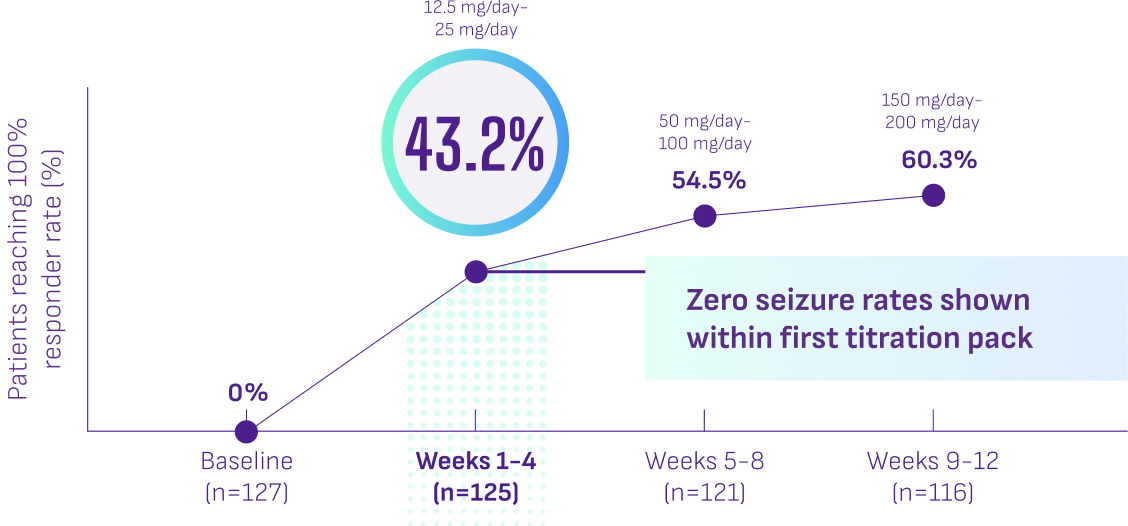
| Zero seizure rates achieved within 4 weeks and increased over time1 |
| Results from a post hoc analysis of a phase 3 study: Percentage of patients with 1-2 seizures/28 days at baseline who achieved zero seizures within the first 4 weeks taking XCOPRI |
|
|
See full study design 
|
| Limitations: This post hoc analysis of an open-label phase 3 study of XCOPRI did not include a control arm. These data are descriptive and representative of an enriched population with a relatively small number of patients. Appropriate multiplicity adjustments were not applied. |
|
|
|
ref-body-eff-002
|
Reference for section "Zero seizure rates achieved within 4 weeks...": 1. Aboumatar S, Biton V, Wechsler R, Ferrari L, Rosenfeld WE. Post hoc analysis of a phase 3 study for treatment of uncontrolled focal seizures: adjunctive cenobamate dose and seizure reduction by baseline seizure frequency. Epilepsy Res. 2022;186:107014.
|
|
|
body-eff-003
| Long-term zero seizure rates seen for 12 months or longer1 |
| Results from a post hoc analysis of a phase 3 study: |
| Zero seizures achieved with XCOPRI regardless of baseline seizure frequency |
|
|
See full study design 
|
| * |
Among patients continuing cenobamate at data cut-off. |
|
| Limitations: This post hoc analysis of an open-label phase 3 study of XCOPRI did not include a control arm. These data are descriptive and representative of an enriched population with a relatively small number of patients. Appropriate multiplicity adjustments were not applied. |
|
|
|
|
|
ref-body-eff-003
|
Reference for section "Long-term zero seizure rates seen...": 1. Aboumatar S, Biton V, Wechsler R, Ferrari L, Rosenfeld WE. Post hoc analysis of a phase 3 study for treatment of uncontrolled focal seizures: adjunctive cenobamate dose and seizure reduction by baseline seizure frequency. Epilepsy Res. 2022;186:107014.
|
|
|
body-eff-004
| Reducing concomitant ASM drug load with XCOPRI |
| Results from a post hoc analysis of a phase 3 study: |
| 62% |
of patients on XCOPRI
discontinued and/or reduced |
| 1 or more ASMs |
| across all drug classes (110/177)1 |
|
|
|
|
| Reducing concomitant ASM drug load with XCOPRI |
| Results from a post hoc analysis of a phase 3 study: |
| 62% |
of patients on XCOPRI
discontinued and/or reduced |
| 1 or more ASMs |
| across all drug classes (110/177)1 |
|
|
|
|
|

|
| In this group of patients, there was no increase or addition of concomitant ASMs.1* |
| The most common concomitant ASMs used at baseline included lacosamide, levetiracetam, lamotrigine, zonisamide, and clobazam.2 |
|
|
| * |
Sodium channel blockers, synaptic vesicle protein 2A ligands, benzodiazepines, and others. |
|
|
ASMs=anti-seizure medications.
|
| Limitations: This post hoc analysis of an open-label phase 3 study of XCOPRI did not include a control arm. These data are descriptive and representative of an enriched population with a relatively small number of patients. Appropriate multiplicity adjustments were not applied. |
|
|
|
|
| In this group of patients, there was no increase or addition of concomitant ASMs.1* |
| The most common concomitant ASMs used at baseline included lacosamide, levetiracetam, lamotrigine, zonisamide, and clobazam.2 |
|
|
| * |
Sodium channel blockers, synaptic vesicle protein 2A ligands, benzodiazepines, and others. |
|
|
ASMs=anti-seizure medications.
|
| Limitations: This post hoc analysis of an open-label phase 3 study of XCOPRI did not include a control arm. These data are descriptive and representative of an enriched population with a relatively small number of patients. Appropriate multiplicity adjustments were not applied. |
|
|
|
|
|
ref-body-eff-004
|
References for section "Reducing concomitant ASM drug load with XCOPRI": 1. Data on file. SK Life Science, Inc. 2. Rosenfeld WE, Abou-Khalil B, Aboumatar S, et al. Post hoc analysis of a phase 3, multicenter, open-label study of cenobamate for treatment of uncontrolled focal seizures: effects of dose adjustments of concomitant antiseizure medications. Epilepsia. 2021;62(12):3016-3028.
|
|
|
body-eff-005
| Switch on XCOPRI sooner |
 |
| #1 branded ASM |
| prescribed by epileptologists* |
 |
| Over 275,000 patients |
| prescribed worldwide and counting† |
 |
| Copay comparable to generics‡ |
| 9 out of 10 Commercial, Medicare, and Medicaid patients have coverage for XCOPRI§ |
 |
| 10+ years of clinical trial and real-world experience |
| Well-studied safety with 5-year retention data1,2 |
|
| #1 branded ASM |
| prescribed by epileptologists* |
|
|
|
| Over 275,000 patients prescribed worldwide and counting† |
|
|
|
| Copay comparable to generics‡ |
| 9 out of 10 Commercial, Medicare, and Medicaid patients have coverage for XCOPRI§ |
|
|
|
| 10+ years of clinical trial and real-world experience |
| Well-studied safety with 5-year retention data1,2 |
|
|
|
| * |
By NBRx, as of July 2025. |
| † |
Worldwide new-to-brand cenobamate prescriptions as of December 2025. Source: IQVIA. |
| ‡ |
IQVIA, Patient Cost Disclosure 12 months ending April 2025. |
| § |
Managed Markets Insight & Technology, LLC, database as of July 2025. |
|
|
|
|
ref-body-eff-005
|
References for section "Switch on XCOPRI sooner": 1. Sander JW, Rosenfeld WE, Halford JJ, Steinhoff BJ, Biton V, Toledo M. Long-term individual retention with cenobamate in adults with focal seizures: pooled data from the clinical development program. Epilepsia. 2022;63(1):139-149. 2. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc.
|
|
|
body-moa-001
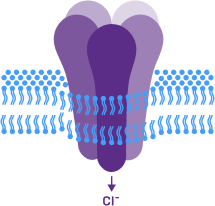
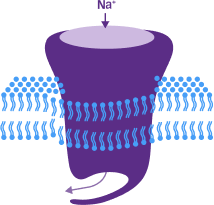
| XCOPRI reduces neuronal excitability through a unique dual MOA1-5* |
| Positive allosteric modulator of the GABAA receptor3,4 |
| Further enhances inhibition by GABAergic neurons |
|
|
| Inhibits persistent sodium current3,5 |
| Preferentially blocks the sodium channel–mediated persistent current |
|
|
| Positive allosteric modulator of the GABAA receptor3,4 |
| Further enhances inhibition by GABAergic neurons |
|
|
|
|
|
| Inhibits persistent sodium current3,5 |
| Preferentially blocks the sodium channel–mediated persistent current |
|
|
|
| Different from other sodium inhibitors, XCOPRI preferentially inhibits persistent sodium current, rather than transient current. XCOPRI also enhances GABAA-mediated inhibition. These are both important targets in epilepsy to maintain balance between excitation and inhibition.1-5 |
| Different from other sodium inhibitors, XCOPRI preferentially inhibits persistent sodium current, rather than transient current. XCOPRI also enhances GABAA-mediated inhibition. These are both important targets in epilepsy to maintain balance between excitation and inhibition.1-5 |
|
| * |
The precise mechanism by which XCOPRI exerts its anticonvulsant activity is unknown.3 |
|
|
|
|
ref-body-moa-001
|
References for section "XCOPRI reduces neuronal excitability...": 1. Guignet M, Campbell A, White HS. Cenobamate (XCOPRI): Can preclinical and clinical evidence provide insight into its mechanism of action? Epilepsia. 2020;61(11):2329-2339. 2. Perucca E, Bialer M, White HS. New GABA-targeting therapies for the treatment of seizures and epilepsy: I. role of GABA as a modulator of seizure activity and recently approved medications acting on the GABA system. CNS Drugs. 2023;37(9):755-779. 3. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc. 4. Sharma R, Nakamura M, Neupane C, et al. Positive allosteric modulation of GABAA receptors by a novel antiepileptic drug cenobamate. Eur J Pharmacol. 2020;879:173117. 5. Nakamura M, Cho JH, Shin H, Jang IS. Effects of cenobamate (YKP3089), a newly developed anti-epileptic drug, on voltage-gated sodium channels in rat hippocampal CA3 neurons. Eur J Pharmacol. 2019;855:175-182.
|
|
|
body-saf-001
10+ years of clinical trial and real-world
experience |
| Over 275,000 patients prescribed worldwide* |

|
| * |
Worldwide new-to-brand cenobamate prescriptions as of December 2025. Source: IQVIA. |
|
|
|
|
|
body-tol-001
| Over 275,000 |
| patients prescribed worldwide and counting* |
| * |
Worldwide new-to-brand cenobamate prescriptions as of December 2025. Source: IQVIA. |
|
|
|
|
body-tol-002
| Cognition with XCOPRI |
 |
| Based on a post hoc analysis of pooled populations across phase 2 and phase 3 studies |
| Rates of cognitive TEAEs observed with XCOPRI were 2.3% vs 0.9% with placebo.1* |
|
| Based on a post hoc analysis of pooled populations across phase 2 and phase 3 studies |
| Rates of cognitive TEAEs observed with XCOPRI were 2.3% vs 0.9% with placebo.1* |
|
|
|
| Limitations: Cognitive symptoms were evaluated using non-standardized measures including spontaneous patient self-reporting, which may have led to underreporting of mild or intermittent symptoms. Baseline cognitive comorbidities were assessed retrospectively and could not be directly compared with TEAEs. Potential confounding effects from concomitant anti-seizure medications further limit interpretation of cognitive findings. |
| * |
Patients with focal epilepsy were assessed on memory impairment, word-finding difficulty, mathematical difficulty, and disturbances in attention. |
|
TEAEs=treatment-emergent adverse events. |
|
|
|
|
ref-body-tol-002
|
Reference for section "Cognition with XCOPRI": 1. Krauss GL, Chung SS, Ferrari L, Stern S, Rosenfeld WE. Cognitive and psychiatric adverse events during adjunctive cenobamate treatment in phase 2 and phase 3 clinical studies. Epilepsy Behav. 2024;151:109605.
|
|
|
body-tol-003
| Weight with XCOPRI |
 |
| Low rates of weight change reported with XCOPRI in pivotal trials1 |
| XCOPRI (3/442) vs placebo (0/216) |
|
| Low rates of weight change reported with XCOPRI in pivotal trials1 |
| XCOPRI (3/442) vs placebo (0/216) |
|
|
|
|
|
|
ref-body-tol-003
|
Reference for section "Weight with XCOPRI": 1. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc.
|
|
|
body-tol-004
| Long-term retention rates1 |
| Pooled data from the clinical development program: |
| At 5 years, the majority of patients remained on treatment |


|
| About the analysis: These retention data are based on Kaplan-Meier estimates of time to discontinuation of open-label XCOPRI in the pooled population from 3 clinical studies. Conclusions of long-term efficacy and safety should not be drawn based on these data. |
| 80% of patients were on 2-3 concomitant anti-seizure medications at the start of open-label XCOPRI treatment. In this pooled population, the median duration of XCOPRI exposure was 2.8 years, with a median XCOPRI modal dose of 200 mg/day. |
|
|
|
ref-body-tol-004
|
Reference for section "Long-term retention rates": 1. Sander JW, Rosenfeld WE, Halford JJ, Steinhoff BJ, Biton V, Toledo M. Long-term individual retention with cenobamate in adults with focal seizures: pooled data from the clinical development program. Epilepsia. 2022;63(1):139-149.
|
|
|
body-dos-001
| Overview of dosing with XCOPRI1 |
 |
| Convenient once-daily dosing and a half-life of 50-60 hours |
|
| Take any time, whole or crushed, with or without food |
|
| Can be taken as monotherapy or adjunctive therapy |
|
| Convenient once-daily dosing and a half-life of 50-60 hours |
|
|
|
| Take any time, whole or crushed, with or without food |
|
|
|
| Can be taken as monotherapy or adjunctive therapy |
|
|
|
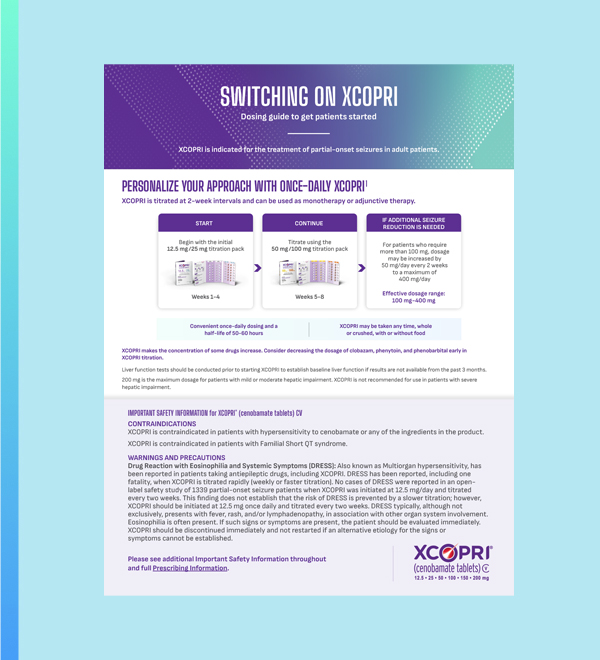
| Liver function tests should be conducted prior to starting XCOPRI to establish baseline liver function if results are not available from the past 3 months. |
| 200 mg is the maximum dosage for patients with mild or moderate hepatic impairment. XCOPRI is not recommended for use in patients with severe hepatic impairment. |
|
|
|
ref-body-dos-001
|
Reference for section "Overview of dosing...": 1. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc.
|
|
|
body-dos-002

|
| Additional blister packs and bottles available. |

|
| Additional blister packs and bottles available. |
|
|
| Flexibility to meet your patients’ unique needs1 |
| • |
Blister packs can simplify the titration schedule when starting XCOPRI |
| • |
Bottles and maintenance blister packs allow for adjustments to find the right dosage for each patient |
|

|
|
|
|
|
ref-body-dos-002
|
Reference for section "Flexibility to meet...": 1. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc.
|
|
|
body-tit-001
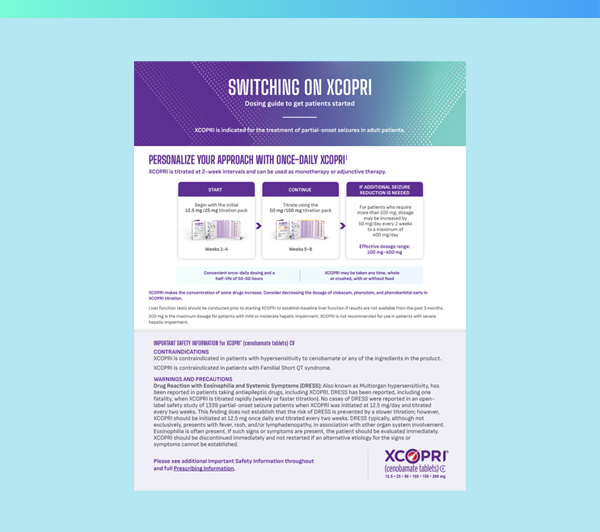
| Personalize your approach with once-daily XCOPRI1 |
| XCOPRI is titrated at 2-week intervals. |
|
|
| • |
Convenient once-daily dosing and a half-life of 50-60 hours |
| • |
Taken any time, whole or crushed, with or without food |
| • |
Can be taken as monotherapy or adjunctive therapy |
|
| Liver function tests should be conducted prior to starting XCOPRI to establish baseline liver function if results are not available from the past 3 months. |
| 200 mg is the maximum dosage for patients with mild or moderate hepatic impairment. XCOPRI is not recommended for use in patients with severe hepatic impairment. |
| * |
Additional blister packs and bottles available. |
|
|
| Flexibility to meet your patients’ unique needs1 |
| • |
Blister packs can simplify the titration schedule when starting XCOPRI |
| • |
Bottles and maintenance blister packs allow for adjustments to find the right dosage for each patient |
|

|
|
|
|
|
ref-body-tit-001
|
Reference for section "Personalize your approach with once-daily XCOPRI": 1. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc.
|
|
|
body-acc-001
| Switch on XCOPRI sooner |
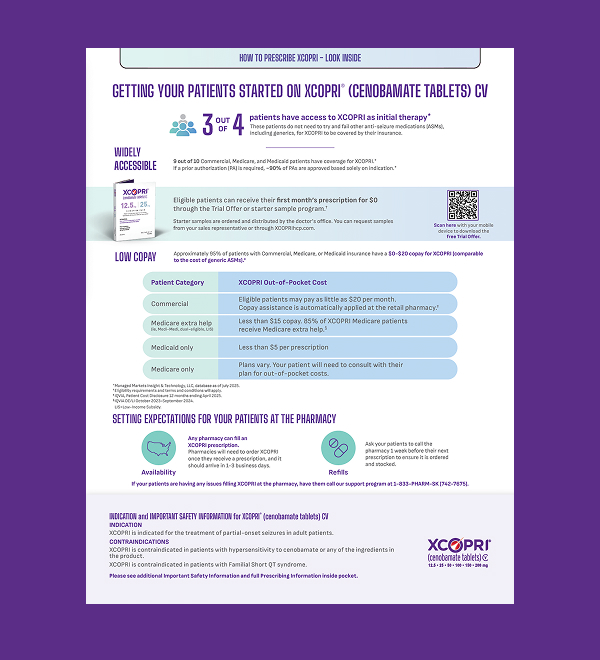
| 3 out of 4 patients have access as initial therapy, meaning they do not need to try and fail other ASMs (including generics) for XCOPRI to be covered by their insurance* |
 |
| Widely accessible |
| 9 out of 10 Commercial, Medicare, and Medicaid patients have coverage for XCOPRI* |
| If a prior authorization (PA) is required, ~90% of PAs are approved based solely on indication* |
 |
| Start at $0 |
| Patients can receive their first month’s prescription for $0 through the Trial Offer or starter sample program† |
 |
| Low copay |
| Approximately 95% of patients with Commercial, Medicare, or Medicaid insurance have a $0-$20 copay for XCOPRI (comparable to the cost of generic ASMs)‡ |
|
| Widely accessible |
| 9 out of 10 Commercial, Medicare, and Medicaid patients have coverage for XCOPRI* |
| If a prior authorization (PA) is required, ~90% of PAs are approved based solely on indication* |
|
|
| Start at $0 |
| Patients can receive their first month’s prescription for $0 through the Trial Offer or starter sample program† |
|
|
|
|
| Low copay |
| Approximately 95% of patients with Commercial, Medicare, or Medicaid insurance have a $0-$20 copay for XCOPRI (comparable to the cost of generic ASMs)‡ |
|
|
|
| * |
Managed Markets Insight & Technology, LLC, database as of July 2025. |
| † |
Eligibility requirements and terms and conditions will apply. |
| ‡ |
IQVIA, Patient Cost Disclosure 12 months ending April 2025. |
|
| ASMs=anti-seizure medications. |
|
|
|
|
body-acc-002
| XCOPRI is widely accessible |
| 9 out of 10 Commercial, Medicare, and Medicaid patients have coverage for XCOPRI.* |

|
| * |
Managed Markets Insight & Technology, LLC, database as of July 2025. |
|

|
| XCOPRI is widely accessible |
| 9 out of 10 Commercial, Medicare, and Medicaid patients have coverage for XCOPRI.* |
|
|
| * |
Managed Markets Insight & Technology, LLC, database as of July 2025. |
|
|
|
|
|
|
|
body-acc-003

|
| Copay comparable to generic ASMs |
| Approximately 95% of patients with Commercial, Medicare, or Medicaid insurance have a $0-$20 copay for XCOPRI.* |

|
| * |
IQVIA, Patient Cost Disclosure 12 months ending April 2025. |
|
|
ASMs=anti-seizure medications. |
|
| Copay comparable to generic ASMs |
| Approximately 95% of patients with Commercial, Medicare, or Medicaid insurance have a $0-$20 copay for XCOPRI.* |
|
|
| * |
IQVIA, Patient Cost Disclosure 12 months ending April 2025. |
|
|
ASMs=anti-seizure medications. |
|
|
|
|
|
|
|
body-acc-004

|
| Covered as first ASM for most patients |
| 3 out of 4 patients have access as initial therapy, meaning they do not need to try and fail other ASMs (including generics) for XCOPRI to be covered by their insurance.* |

|
| * |
Managed Markets Insight & Technology, LLC, database as of July 2025. |
|
|
ASM=anti-seizure medication. |
|
| Covered as first ASM for most patients |
| 3 out of 4 patients have access as initial therapy, meaning they do not need to try and fail other ASMs (including generics) for XCOPRI to be covered by their insurance.* |
|
|
| * |
Managed Markets Insight & Technology, LLC, database as of July 2025. |
|
|
ASM=anti-seizure medication. |
|
|
|
|
|
|
|
body-acc-005
| XCOPRI is available for convenient home delivery through Amazon Pharmacy |
| E-scribe XCOPRI right to Amazon Pharmacy, just like any other pharmacy. |

|
|
|
|
|
|
body-acc-006
| XCOPRI is available to order at all pharmacies |
| Need additional support? |
| We’re here to help your patients get started on XCOPRI and stay on with a variety of support services. |

|
|
|
|
|
|
body-acc-007
| Get support with SK Life Science Navigator |
| For patients |
| • |
Free product to eligible patients who are uninsured, underinsured, or experiencing financial hardship |
| • |
Help to locate XCOPRI if your patient’s local pharmacy does not have it in stock |
|
| For your practice |
| • |
Help to identify whether a patient’s insurance plan covers XCOPRI |
| • |
If a PA is required, SKLSI Navigator will provide the information that is needed |
| • |
Downloadable sample letter of appeal, medical necessity, and more |
|
|
PA=prior authorization; SKLSI=SK Life Science, Inc. |
|

|
|
|
|
|
body-acc-008
| Specialty pharmacies can help get quick access to XCOPRI and PA support |
 |
| Convenient home delivery, including urgent or emergency requests |
|
|
| Refill reminders |
|
|
| Resolving PA requests |
|
|
|
Convenient home delivery, including urgent or emergency requests |
|
|
Refill reminders |
|
|
Resolving PA requests |
|
|
|
|
|

|
|
|
|
|
|
body-gen-001
| XCOPRI resources and downloadable tools for your patients and practice |
 |
| Expert insights |
| Hear from your peers who have switched on the power of XCOPRI—and are seeing meaningful results. |

|
|
|
| Expert insights |
| Hear from your peers who have switched on the power of XCOPRI—and are seeing meaningful results. |
|
|
|
|
 |
| XCOPRI patients |
| Real patients. Real progress. See how XCOPRI is helping light the way forward to fewer seizures. |

|
|
|
| XCOPRI patients |
| Real patients. Real progress. See how XCOPRI is helping light the way forward to fewer seizures. |
|
|
|
|
 |
| Downloadable PDFs |
| Our clinical resources and patient support tools are designed to help you make informed decisions, every step of the way. |

|
|
|
| Downloadable PDFs |
| Our clinical resources and patient support tools are designed to help you make informed decisions, every step of the way. |
|
|
|
|
 |
| FAQs |
| Explore answers to common questions about XCOPRI. |

|
|
|
| FAQs |
| Explore answers to common questions about XCOPRI. |
|
|
|
|
|
|
|
cta-urg-001
|
See why a chance at zero seizures can’t wait.
|

|
|
|
|
|
cta-eff-001
Discover the power of once-daily
XCOPRI.1
|

|
|
|
|
|
ref-cta-eff-001
|
Reference for section "Discover the power...": 1. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc.
|
|
|
cta-moa-001
|
See how the XCOPRI MOA differs from other sodium inhibitors.1-5
|

|
|
|
|
|
|
|
ref-cta-moa-001
|
References for CTA "See how the XCOPRI MOA...": 1. Guignet M, Campbell A, White HS. Cenobamate (XCOPRI): Can preclinical and clinical evidence provide insight into its mechanism of action? Epilepsia. 2020;61(11):2329-2339. 2. Perucca E, Bialer M, White HS. New GABA-targeting therapies for the treatment of seizures and epilepsy: I. role of GABA as a modulator of seizure activity and recently approved medications acting on the GABA system. CNS Drugs. 2023;37(9):755-779. 3. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc. 4. Sharma R, Nakamura M, Neupane C, et al. Positive allosteric modulation of GABAA receptors by a novel antiepileptic drug cenobamate. Eur J Pharmacol. 2020;879:173117. 5. Nakamura M, Cho JH, Shin H, Jang IS. Effects of cenobamate (YKP3089), a newly developed anti-epileptic drug, on voltage-gated sodium channels in rat hippocampal CA3 neurons. Eur J Pharmacol. 2019;855:175-182.
|
|
|
cta-saf-001
|
See the 10+ years of clinical trial and real-world experience with XCOPRI.
|
|
|

|
|
|
|
cta-tol-001
Well-studied safety:
See XCOPRI clinical trial data.1
|

|
|
|
|
|
|
|
ref-cta-tol-001
|
Reference for CTA "Well-studied safety...": 1. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc.
|
|
|
cta-dos-001
|
XCOPRI offers once-daily dosing with a personalized treatment approach.1
|

|
|
|
|
|
ref-cta-dos-001
|
Reference for CTA “XCOPRI offers once-daily dosing...” 1. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc.
|
|
|
cta-tit-001
|
Learn about convenient blister packs to help patients start and stay on XCOPRI.1
|
|
|
|
|
|
Learn about convenient blister packs to help patients start and stay on XCOPRI.1
|
|
|
|
|
|
|
ref-cta-tit-001
|
Reference for CTA "Learn about convenient blister...": 1. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc.
|
|
|
cta-acc-001
|
Starting a patient on XCOPRI? Get the access information you need.
|

|
|
|
|
|
cta-gen-001
|
Explore tools for your patients and practice.
|

|
|
|
|
Explore tools for your patients and practice.
|
|
|
|
|
|
|
cta-gen-002
| Getting Patients Started on XCOPRI Guide |
| Get guidance on coverage, prescribing XCOPRI, and support programs for your practice and patients. |

|
|
|
|
| Getting Patients Started on XCOPRI Guide |
| Get guidance on coverage, prescribing XCOPRI, and support programs for your practice and patients. |
|
|
|
|
|
|
|
|
cta-gen-003
| Switching On XCOPRI Flashcard |
| Find important information about prescribing XCOPRI, how to titrate, and drug load reduction. |

|
|
|
|
| Switching On XCOPRI Flashcard |
| Find important information about prescribing XCOPRI, how to titrate, and drug load reduction. |
|
|
|
|
|
|
|
|
cta-gen-004
| For patients: XCOPRI Brochure |
| This brochure includes information for patients on how to take XCOPRI, potential side effects, and a patient-friendly version of XCOPRI study data. |

|
|
|
|
| For patients: XCOPRI Brochure |
| This brochure includes information for patients on how to take XCOPRI, potential side effects, and a patient-friendly version of XCOPRI study data. |
|
|
|
|
|
|
|
|
cta-gen-005
|
|
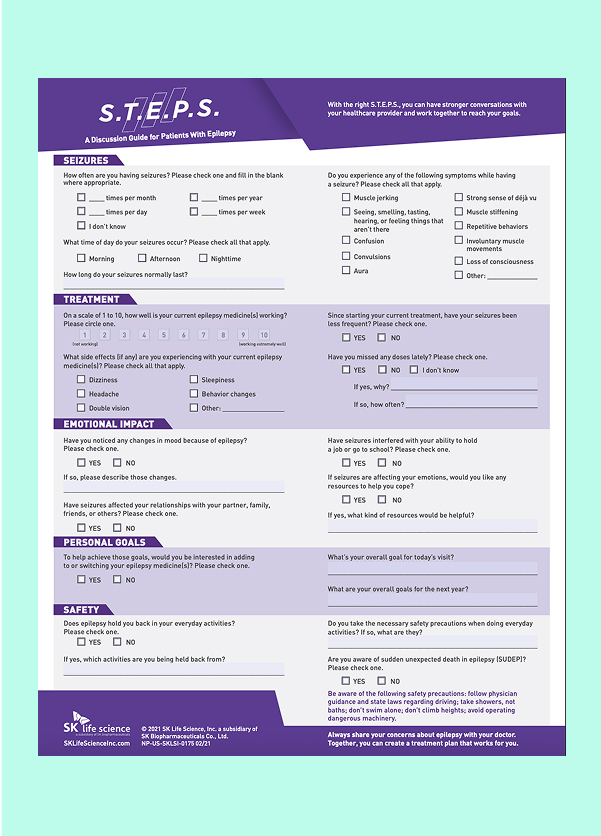
| For patients: S.T.E.P.S. Discussion Guide |
| Based on a survey of patients, caregivers, and healthcare providers, this guide is designed to help foster the patient/care team relationship and help patients reach their goals. Available in English and Spanish. |

|
|
|
|
| For patients: S.T.E.P.S. Discussion Guide |
| Based on a survey of patients, caregivers, and healthcare providers, this guide is designed to help foster the patient/care team relationship and help patients reach their goals. Available in English and Spanish. |
|
|
|
|
|
|
|
|
|
cta-gen-006
| For patients: Next Steps Brochure |
| This brochure helps patients understand what to expect when starting XCOPRI, including guidance on filling their prescription, copay information, support programs, potential side effects, and patient testimonials. |

|
|
|
|
| For patients: Next Steps Brochure |
| This brochure helps patients understand what to expect when starting XCOPRI, including guidance on filling their prescription, copay information, support programs, potential side effects, and patient testimonials. |
|
|
|
|
|
|
|
|
|
cta-moa-002
| See how XCOPRI works |
| Key opinion leader Dr. Raman Sankar explains how XCOPRI reduces neuronal excitability through a dual mechanism of action.1-5* |

|
| * |
The precise mechanism by which XCOPRI exerts its anticonvulsant activity is unknown.3 |
|
|
|
|
| See how XCOPRI works |
| Key opinion leader Dr. Raman Sankar explains how XCOPRI reduces neuronal excitability through a dual mechanism of action.1-5* |
|
|
| * |
The precise mechanism by which XCOPRI exerts its anticonvulsant activity is unknown.3 |
|
|
|
|
|
|
|
|
ref-cta-moa-002
|
References for section "See how XCOPRI works": 1. Guignet M, Campbell A, White HS. Cenobamate (XCOPRI): Can preclinical and clinical evidence provide insight into its mechanism of action? Epilepsia. 2020;61(11):2329-2339. 2. Perucca E, Bialer M, White HS. New GABA-targeting therapies for the treatment of seizures and epilepsy: I. role of GABA as a modulator of seizure activity and recently approved medications acting on the GABA system. CNS Drugs. 2023;37(9):755-779. 3. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc. 4. Sharma R, Nakamura M, Neupane C, et al. Positive allosteric modulation of GABAA receptors by a novel antiepileptic drug cenobamate. Eur J Pharmacol. 2020;879:173117. 5. Nakamura M, Cho JH, Shin H, Jang IS. Effects of cenobamate (YKP3089), a newly developed antiepileptic drug, on voltage-gated sodium channels in rat hippocampal CA3 neurons. Eur J Pharmacol. 2019;855:175-182.
|
|
|
utility-end-001
Primary Outcome
In a study with adult patients with a median of 9 seizures/28 days at baseline, patients taking XCOPRI experienced up to 2x greater seizure reduction compared with placebo (55% XCOPRI 400 mg, 55% XCOPRI 200 mg, 36% XCOPRI 100 mg vs 24% placebo).1,2
|
|
|
|
ref-utility-end-001
|
References for Primary Outcome: 1. Krauss GL, Klein P, Brandt C, et al. Safety and efficacy of adjunctive cenobamate (YKP3089) in patients with uncontrolled focal seizures: a multicentre, double-blind, randomised, placebo-controlled, dose-response trial. Lancet Neurol. 2020;19(1):38-48. 2. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc.
|
|
|
utility-end-002
Secondary Outcome
In a study with adult patients with a median of 9 seizures/28 days at baseline, as many as 1 in 5 experienced zero seizures with XCOPRI during the maintenance phase (21% XCOPRI 400 mg, 11% XCOPRI 200 mg, 4% XCOPRI 100 mg, 1% placebo).1,2
|
|
|
|
ref-utility-end-002
|
References for Secondary Outcome: 1. Krauss GL, Klein P, Brandt C, et al. Safety and efficacy of adjunctive cenobamate (YKP3089) in patients with uncontrolled focal seizures: a multicentre, double-blind, randomised, placebo-controlled, dose-response trial. Lancet Neurol. 2020;19(1):38-48. 2. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc.
|
|
|
utility-end-003
Primary and Secondary Outcomes
In a study with adult patients with a median of 9 seizures/28 days at baseline, patients taking XCOPRI experienced up to 2x greater seizure reduction compared with placebo (55% XCOPRI 400 mg, 55% XCOPRI 200 mg, 36% XCOPRI 100 mg vs 24% placebo). In the same group of patients, as many as 1 in 5 experienced zero seizures with XCOPRI during the maintenance phase (21% XCOPRI 400 mg, 11% XCOPRI 200 mg, 4% XCOPRI 100 mg, 1% placebo).1,2
|
|
|
|
ref-utility-end-003
|
References for Primary and Secondary Outcomes: 1. Krauss GL, Klein P, Brandt C, et al. Safety and efficacy of adjunctive cenobamate (YKP3089) in patients with uncontrolled focal seizures: a multicentre, double-blind, randomised, placebo-controlled, dose-response trial. Lancet Neurol. 2020;19(1):38-48. 2. XCOPRI [package insert]. Paramus, NJ: SK Life Science, Inc.
|
|
|
utility-isipre-001
|
INDICATION and IMPORTANT SAFETY INFORMATION for XCOPRI® (cenobamate tablets) CV
|
INDICATION
XCOPRI is indicated for the treatment of partial-onset seizures in adult patients.
|
CONTRAINDICATIONS
XCOPRI is contraindicated in patients with hypersensitivity to cenobamate or any of the ingredients in the product.
|
|
XCOPRI is contraindicated in patients with Familial Short QT syndrome.
|
|
See below for additional Important Safety Information and full Prescribing Information.
|
|
|
|
utility-isipre-002
|
IMPORTANT SAFETY INFORMATION for XCOPRI® (cenobamate tablets) CV
|
CONTRAINDICATIONS
XCOPRI is contraindicated in patients with hypersensitivity to cenobamate or any of the ingredients in the product.
|
|
XCOPRI is contraindicated in patients with Familial Short QT syndrome.
|
|
See below for additional Important Safety Information and full Prescribing Information.
|
|
|
|
utility-isi-001
|
IMPORTANT SAFETY INFORMATION and INDICATION for XCOPRI® (cenobamate tablets) CV
|
CONTRAINDICATIONS
XCOPRI is contraindicated in patients with hypersensitivity to cenobamate or any of the ingredients in the product.
|
|
XCOPRI is contraindicated in patients with Familial Short QT syndrome.
|
WARNINGS AND PRECAUTIONS
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS): Also known as Multiorgan hypersensitivity, has been reported in patients taking antiepileptic drugs, including XCOPRI. DRESS has been reported, including one fatality, when XCOPRI is titrated rapidly (weekly or faster titration). No cases of DRESS were reported in an open-label safety study of 1339 partial-onset seizure patients when XCOPRI was initiated at 12.5 mg/day and titrated every two weeks. This finding does not establish that the risk of DRESS is prevented by a slower titration; however, XCOPRI should be initiated at 12.5 mg once daily and titrated every two weeks. DRESS typically, although not exclusively, presents with fever, rash, and/or lymphadenopathy, in association with other organ system involvement. Eosinophilia is often present. If such signs or symptoms are present, the patient should be evaluated immediately. XCOPRI should be discontinued immediately and not restarted if an alternative etiology for the signs or symptoms cannot be established.
|
|
QT Shortening: XCOPRI can cause shortening of the QT interval. Caution should be used when administering XCOPRI and other drugs that shorten the QT interval as there may be a synergistic effect on the QT interval that would increase the QT shortening risk.
|
|
Suicidal Behavior and Ideation: Antiepileptic drugs (AEDs), including XCOPRI, increase the risk of suicidal thoughts or behavior in patients taking these drugs for any indication. Patients treated with any AED for any indication should be monitored for the emergence or worsening of depression, suicidal thoughts or behavior, and/or any unusual changes in mood or behavior. Advise patients, their caregivers, and/or families to be alert for these behavioral changes and report them immediately to a healthcare provider.
|
|
Liver Injury: Clinically significant liver injury has occurred in patients taking XCOPRI. Obtain serum transaminases (ALT and AST) and total bilirubin, if not recently available (i.e., within 3 months) before initiating XCOPRI, and during treatment if clinically indicated. Monitor patients for signs and symptoms of any hepatic injury during treatment. Discontinue XCOPRI in patients with evidence of liver injury in the absence of an alternative etiology.
|
|
Neurological Adverse Reactions: XCOPRI can cause dose-dependent increases in the neurologic adverse reactions including dizziness, diplopia, disturbance in gait and coordination, somnolence, and fatigue.
|
|
Prescribers should advise patients against engaging in hazardous activities requiring mental alertness, such as operating motor vehicles or dangerous machinery, until the effect of XCOPRI is known.
|
|
Withdrawal of AEDs: As with all antiepileptic drugs, XCOPRI should generally be withdrawn gradually because of the risk of increased seizure frequency and status epilepticus. If withdrawal is needed because of a serious adverse event, rapid discontinuation can be considered.
|
MOST COMMON ADVERSE REACTIONS
In adult adjunctive therapy placebo-controlled clinical studies, the most common adverse reactions that occurred in XCOPRI-treated patients (incidence at least 10% and greater than placebo) were somnolence, dizziness, fatigue, diplopia, headache.
|
DOSING CONSIDERATIONS
Dosage adjustment of XCOPRI or other concomitant medications may be necessary.
|
| • |
Consider gradually reducing phenytoin dosages by up to 50% during initial titration. |
| • |
Consider reducing dosages of phenobarbital and clobazam as needed when used concomitantly with XCOPRI. |
| • |
When XCOPRI and carbamazepine or lamotrigine are taken concomitantly, consider increasing dosages as needed of carbamazepine or lamotrigine. |
| • |
Consider increasing dosages as needed of drugs which are CYP2B6 and CYP3A substrates and decreasing dosages as needed of drugs which are CYP2C19 substrates. |
| • |
Effectiveness of hormonal oral contraceptives may be reduced when administered concomitantly with XCOPRI. Women should use additional or alternative non-hormonal birth control. |
|
|
Dosage reduction of XCOPRI may be considered in patients with mild to moderate and severe renal impairment. XCOPRI is not recommended in end‑stage renal disease.
|
|
The maximum recommended daily dose is 200 mg for patients with mild or moderate hepatic impairment. XCOPRI is not recommended in patients with severe hepatic impairment.
|
DRUG ABUSE
XCOPRI is a Schedule V controlled substance.
|
INDICATION
XCOPRI is indicated for the treatment of partial-onset seizures in adult patients.
|
|
Please see full Prescribing Information.
|
|
|
|
utility-foot-001
|
If you no longer wish to receive email communications from XCOPRI, please unsubscribe or manage your communication preferences.
|
|
SK Life Science, Inc.
461 From Road
Paramus, NJ 07652
Tel: 1-201-421-3800
|
© 2026 SK Life Science, Inc., a subsidiary of SK Biopharmaceuticals Co., Ltd.
PM-US-XCOP-1398 4/26
|
|
|
SK Life Science, Inc.
461 From Road
Paramus, NJ 07652
Tel: 1-201-421-3800
|
© 2026 SK Life Science, Inc., a subsidiary of SK Biopharmaceuticals Co., Ltd.
PM-US-XCOP-1398 4/26
|
|
|
|
|
|